Assessing Intra-Community Public Health Impacts from Compounding Food, Energy, and Water Insecurities
Publication Date: 2023
Abstract
Puerto Rico recurrently experiences compounding and interacting climatic- and non-climatic hazards. These diverse hazards (e.g., hurricanes, earthquakes, pandemic) pose complex risks within and across interconnected food, energy, and water (FEW) systems—resulting in significant and adverse public health outcomes. This project extended research from our earlier Public Health Disaster Research Award, which we documented in the report, Social Capital, Community Health Resilience, and Compounding Hazards in Corcovada, Puerto Rico. For this study, we developed, piloted, and validated a problem-focused, solutions-oriented, and community-centered survey in Corcovada, Puerto Rico, which assesses household FEW insecurity experiences and associated health risks before, during, and after single and compounding hazards. Many existing public health assessments focus only on food- or water-related challenges under individual hazard contexts, failing to capture the complexity or magnitude of health risks experienced by communities facing diverse climatic and non-climatic hazards that impact interconnected food, energy, and water systems. The co-creation of the survey has significant public health implications including early identification of at-risk populations, monitoring health outcomes in the community, and informing disaster preparedness, response and mitigation plans. Future research involves scaling the survey across Puerto Rico and beyond for use by local communities’ leaders and public health officials.
Introduction
Recent research on the human dimensions of climate change emphasizes the inadequacy of examining single climatic stressors, instead stressing the need to evaluate the compounding climatic- and non-climatic risks that communities—especially those at the frontlines of climate change impacts—experience (e.g., Zscheischler et al., 20181; Zscheischler et al., 20202; Thomas et al., 20203; Intergovernmental Panel on Climate Change, 20214). Puerto Rico recently experienced several major socio-environmental hazard events, including Hurricane María in 2017, the 2020 earthquakes, the COVID-19 pandemic, and most recently, Hurricane Fiona in 2022—all within a span of five years. Therefore, disaster risk reduction and response efforts must be attentive to the elevated risks that emerge from a diversity of compounding and interacting hazards on public health and critical resources.
In our previous Public Health Report, Social Capital, Community Health Resilience, and Compounding Hazards in Corcovada, Puerto Rico (Roque et al., 20225), we examined the multitude of public health-related risks associated with compounding hazards and their cascading impacts on food, energy, and water (FEW) systems. For this Continuation Award, we draw from the data collection and experience to co-develop and pilot a survey with community members of Corcovada, Puerto Rico. The survey, through three modules, is designed to be used by community leaders, public health professionals and related stakeholders before, during, and/or after hazards to gauge the associated FEW insecurities and their impacts on residents’ public health.
We developed this survey instrument through a series of validation processes, including consulting academic experts in food, water, and energy security, and in partnership with community experts in Corcovada. We then piloted a “survey of the survey,” for the “before hazard” version of the survey through face-to-face, household interviews, in the case study area. This allowed the research team to identify unclear language and receptivity from participants with the survey objectives. However, the pilot was just one component of survey development, as the instrument built from the direct feedback of community members in two community events, one before survey development, which informed the initial survey construction, and one after, which provided additional direct feedback on the pilot instrument and other survey-related issues. This report elaborates on the processes and outcomes of community survey design, validation, and initial results of the pilot instrument.
Literature Review
Single and compounding climatic hazards interact with the social and built environments, challenging critical resource systems, such as food, energy, and water (Dargin et al., 20206; Wells et al., 20227). The disruption of these interconnected systems increases the household-level risks of FEW insecurity, posing adverse health outcomes. For example, household food insecurity is associated with iron deficiencies, malnutrition, and adverse mental health outcomes (Ashby et al., 20168; Eicher-Miller et al., 20099); household water insecurity is associated with emotional distress (e.g., Wutich & Ragsdale, 200810; Sultana, 201111; Wutich et al., 202012; Brewis et al., 202113), illnesses and infections (Rosinger, 201814; Rosinger & Young, 202015; Stoler et al., 202116); and household energy insecurity deepens food and water stress while further contributing to a range of adverse health outcomes (e.g. sleep loss, respiratory illness, and mental health issues) (Hernández, 201317).
FEW security is central in both public health and disaster-related studies (Roque et al., 2022), as it presents challenges in understanding the association between public health impacts during and after disasters. For example, post-disaster power outages can challenge water availability and quality, in turn limiting healthy food choices (Lopez-Cardalda et al., 201818; Clay, 202219). Such interdependencies underscore the need for “nexus” thinking (Daher et al., 202120), which can heighten integrative attention toward preparing, adapting, and mitigating FEW insecurities (Schmidt et al., 202221).
Several assessment tools exist to evaluate household experiences with individual dimensions of food, energy, or water insecurity. For example, the U.S. Department of Agriculture (201222) Household Food Security Scale Module is a validated survey used to monitor food insecurity experiences in the United States. The Household Water Insecurity Experience Scale (Young et al., 201923) and the National Health Interview Survey (Botman & Moriarity, 200024) are other sets of examples. Others developed household energy insecurity scales (e.g., Cook et al. 200825; Colton et al., 200826; Boateng et al., 202027). However, these instruments advance our understanding of food, energy, and water insecurities largely independently (Brewis et al., 202028). They are unable to provide insight into interactive food, energy, and water insecurities. That is, existing standardized instruments do not conceptualize and measure food, energy, and water insecurities as non-independent. This limits our collective understanding of the combined impacts of these insecurities on public health, which is critical during post-disaster periods where health risks are heightened.
Existing public health assessment tools—such as the Community Assessment for Public Health Emergency Response (CASPER, Centers for Disease Control and Prevention, 201929; Schnall et al., 201730), the Environmental Health Shelter Assessment Tool (McDavid & Cruz, 201931), and the Disaster-Related Mortality Surveillance Form (Noe, 201832)—are useful in assessing health challenges after a disaster (e.g., food and water-borne disease, physical injury, psychological impacts, morbidity, and mortality). While these instruments contribute to understanding community health resilience, such instruments are intended to be deployed by public health officials, emergency managers, or academics. To our knowledge no tools exist for local leaders, who seek to document their own public health experiences, yet do not have the technical expertise needed to use existing assessment tools.
Community leaders and other local stakeholders often bear central responsibilities for disaster management (Lillibridge et al., 199333). During and after disasters, communities often rely on their social networks and community organizing to meet their food, water, energy, and health needs (Roque, et al., 202134; Vega, 201935; Mulligan & Garriga-Lopez, 202136). Usable and comprehensive assessments remain urgent for advancing community health resilience, community emergency management organizing, education, and advocacy at local and state levels given the role of these community leaders.
Research Questions
Considering literature gaps, the research questions guiding this project are the following:
- How can communities understand the interacting and reinforcing impacts of FEW insecurities and their associated public health outcomes through an efficient and easily administered survey?
- How might input from community experts and participants shape the design and useability of the survey, and the potential knowledge production and risk reduction strategies learned?
Survey Design Methods
This survey design section explains how our research team co-developed an original survey with community leaders from Corcovada, Puerto Rico, which could later be used by community leaders to assess FEW insecurities and community health in disaster contexts. Figure 1 presents a timeline of our research activities and each step in the survey development process.
Figure 1. Research Activities Timeline and Survey Development Process
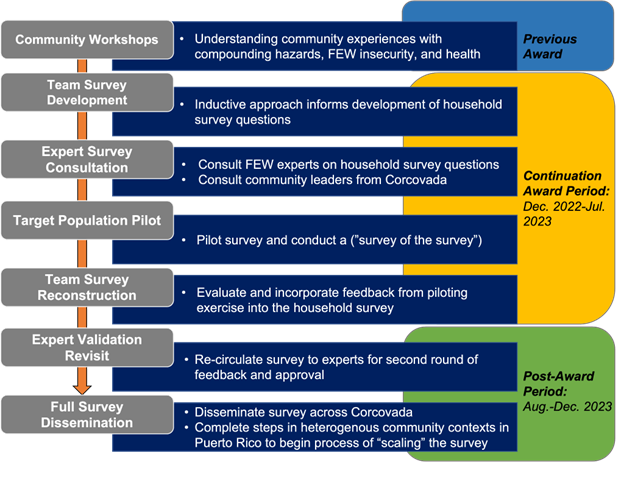
To create, validate, and pilot our survey, we used an initial three-step process, with more specific steps presented in Figure 1. This approach is similar to other survey creation and validation utilizing a community-based participatory research approach (CBPR) (see Kelley et al., 201937). First, we continued the research undertaken in Special Call 2: Strengthening Community Resilience in the U.S. Territories, where we hosted a two-day workshop with community leaders in Corcovada to explore the interlinkages between compounding hazards, social capital, and public health resilience (Roque et al., 2022). We prompted community leaders to identify questions and areas of concern for their community focusing on challenges across food, energy, water, and community health.
The first step of our project—depicted by the first box in Figure 1—was “Team Survey Development.” This phase of the project drew from workshop data from our ongoing community-based participatory research as well as the FEW (in)security and emergency public health literature. This was an inductive and exploratory data analysis approach that allowed our research team to develop the survey questions pertaining to FEW securities and community health, public health practices, and demographic variables. This phase of the project required the research team (co-authors) to meet regularly to develop questions in different iterations, as well as constructing “survey of the survey” questions for academics and community experts.
During this initial phase, our research team decided to develop a survey with three modules: before hazard module (1-2 years before/after a disaster declaration), during disaster module (within 3 months), and after a disaster or natural hazard module (after 6 months). We chose the three-module format because it will enable community leaders to assess highly context-specific needs in different temporal periods of a disaster or hazard in order to prepare and respond to public health outcomes. This survey and its modules will serve various functions for community leaders. These include allowing them to identify where to focus their mutual aid efforts, community health monitoring, as well as articulate community disaster resilience, preparedness, and recovery needs in communication and grantmaking efforts with funders. Further, the use of these surveys could support efforts to prevent extractive activities from researchers that tend to descend on disaster-stricken communities shortly after disasters without understanding local needs, while also building lasting relationships with local communities. Within this context, this tool can support community leaders in capturing the main aspects of information that they need regarding aid and redirect external aid more adequately. To this end, we intentionally made the survey accessible linguistically by using colloquial language. At the end of this phase, our team had prepared a full first draft of the survey in English and Spanish.
In step two, the “Expert Survey Consultation” phase, we used expert consultation to validate the initial survey questions for accuracy, bias, and clarity. We consulted two groups of experts: (1) academic experts in food, water, and energy with field research experience that included household surveys and (2) community experts from Corcovada, Puerto Rico, who previously worked with us on community-based research and had firsthand experience addressing issues of food, energy, water insecurity and health following disasters for feedback on clarity of questions. We consulted three academic experts who specialized in food-, energy-, or water-security, respectively, as well as four community experts for the first round of review. Then, we incorporated the feedback from both academic and community experts, adjusting language, question order, adding examples for clarity, and changing questions for consistency across the modules.
In the third step, “Target Population Pilot,” we piloted the “before hazard” module survey with a specific target population in Corcovada (n=13). We chose to use only the “before hazard” module because (1) there was no current nor post-disaster in the time of the deployment of the test pilot, (2) the modules are streamlined so problems found in one can be fixed in others, and (3) only using one module saved time and helped to avoid participant fatigue. In addition to the survey module questions, we also asked respondents to rate their understanding of questions and describe any thoughts they had about the survey. Since two-thirds of the population rely on a water aqueduct system and the community is predominantly elderly (Roque et al., 2022; Asencio-Yace, 202038), we used a convenience sample approach to maximize variability across age, gender, and household composition (e.g., head of household with children, elder living alone, no access to community water aqueduct). We deployed the survey with 13 residents and reached data saturation (i.e., no new feedback was received). Interviews lasted between 25-45 minutes. The pilot asked respondents about comprehension and relevance of key terms used in the survey, with clarifying questions on FEW securities, if the questions reflected their lived situation, comfortability if a community leader would come to collect this type of data and if there are any critical resources or infrastructure failures missing that are important to their livelihoods.
In the fourth step, Team Survey Reconstruction consisted of the co-author team meeting for two 2-hour long meetings to review and incorporate feedback from academic and community experts. One person on the team reviewed each document with feedback as another co-author incorporated that feedback into both the English and Spanish versions of the survey. Team members also discussed and democratically decided on any changes that had outstanding questions. Following the feedback from community members at the July 17, 2023, community event, we will incorporate this into the reconstruction of the survey (see Figure 1, “Team Survey Reconstruction”). Beyond the scope of this project, we will complete another round of expert validation with both academic and community leaders (Figure 1, “Expert Validation Revisit”) before disseminating the survey at a population-level within the community of Corcovada (Figure 1, “Full Survey Dissemination”).
Findings
Team Survey Development Outcomes
The overarching goal of this project was to develop an accessible and action-oriented instrument for community leaders and public health practitioners. As such, the FEW security questions sought to address the availability, reliability, accessibility, and quality of food, energy, and water, but were very different depending on the survey’s timing (before, during, and after) in the initial survey creation. The public health questions focused on community health which included questions on identifying special health care needs in the household (e.g., equipment, family members with special needs), environmental health (e.g., water quality), mental health, and emergency health preparedness amongst others. Additionally, we noticed that most of our questions were closed ended and health questions were very specific (e.g., are any family members bedridden?). Considering the action-oriented focus of the survey, we agreed—at first—this would allow for easy collection and data analysis. Considering the food, energy, water and health nexus, we expanded health questions to have explicit connections to energy, food, and water (e.g., electricity dependence for health equipment, dietary restrictions due to health and water source for drinking and sanitation). For expert consultation, the research team shared the survey via email and allowed two weeks for feedback through track-changes or notes. This email included a set of questions to elaborate their feedback. Following this, the research team met with them via zoom or in person to have a detailed discussion on their feedback. This included wording, clarity, question order, question sensitivity, and a space for other comments.
Expert Feedback Outcomes
The academic and community experts recommended several ways to improve the clarity and consistency of the survey. First, they recommended that questions in the three modules (before, during, and after) have a consistent flow so that community leaders and public health officials could compare variation across modules. To fix this, we used consistent questions and question-wording to create a better flow throughout the instrument. We also fixed grammar and numbering across the survey. After incorporating both academic and community expert feedback, each module in the survey was 40 questions and had streamlined questions across modules.
One challenge we encountered is that academic and community experts often varied in their feedback, sometimes contradicting one another. For example, academics were more concerned with the confidentiality aspect of the survey (e.g., who is going to have access to the information) while community leaders appreciated that we did not ask about income, which is usually left until the end of surveys due to question sensitivity. Further, community leaders did not mind the demographic questions at the beginning of the survey, which academics usually place at the end for fear of participants leaving the survey from the sensitivity of these questions. This was also reflected in the findings of the initial test pilot, as no interviewees expressed any concerns about the demographic questions. Overall, community experts were not concerned about confidentiality or data access thus challenging academics’ hesitation on this end. Community experts also preferred open-ended questions that would allow respondents to expand on specific topics. Overall, academics focused on the nuance that the survey needed to capture to inform theory. In contrast, the community leaders focused on how the survey would be useful for assessing and meeting community needs, showcasing the necessity of consulting communities to gain their perspective.
Target Population Pilot Outcomes
The test pilot of the “before” module was conducted with 13 households at the time of this report and shows receptiveness from participants. However, there were concerns about question structure and unrecognizable words. One participant did not fully understand some words used in the survey, such as what was meant by a motor vehicle (vehículo motorizado) and also suggested some clearer ways to word questions. Others found gaps in questions, such as not having an option for if there were no health concerns in a household or if a household does not have any immediate neighbors. This feedback was specific and provided insight on how to improve certain questions not considered by the research team, community experts, or academic experts.
Conclusions
This research enabled us—together with our partners in Corcovada—to co-create a public health assessment tool that communities can use to address FEW insecurities and health issues before, during, and after disasters. While local leaders understand how these insecurities manifest in their communities before and after crises, this survey will allow them to easily quantify how many households are experiencing FEW insecurities (i.e., accessibility, reliability, quality, availability) and to identify those in need of assistance in ways that better target aid efforts. This survey will also allow for users to collect data and draw conclusions for action efficiently, as this survey considers the interacting and reinforcing impact of FEW insecurities and related public health risks.
We sought to develop an action-oriented survey with input from community experts and residents as an essential part of this process. Collaborating with community experts and residents provided culturally relevant insights relating to their experiences with these insecurities. Since community leaders may not have higher education training or have challenges with technology, we focus on developing a survey that could be both easy to administer as well as easy for data analysis. This is expected to facilitate data analysis and dissemination of results to different forums (e.g., local organizations, emergency preparedness plans). Overall, the co-creation of this survey can inform those with resources, such as local governments, federal agencies, emergency managers, non-profits, or other organizations, how best to aid before, during, and after a disaster event. Such an approach is intended to contribute to community-based and community-driven public health initiatives and support.
Our survey innovates by including questions related to chronic conditions, disability, and mental health/mental distress which is a significant step toward addressing the unique vulnerabilities of individuals in disaster-prone areas like Puerto Rico. By identifying these specific household health vulnerabilities, community leaders and decision-makers can gain valuable insights to inform their disaster planning and response strategies. This approach is especially important in Puerto Rico, considering its aging population (median age is 44.2 vs 38.8 in the United States) and the increasing prevalence of self-reported poor physical and mental health status, and depression diagnoses following Hurricane María in 2017. (Chandra et al., 202139). Our co-created survey assists community leaders at the intersection of compounding hazards and public health by providing tools to know and understand community gaps and needs.
Public Health Implications
This report highlights the importance of co-creating public health surveys and assessments with diverse stakeholders. Co-creation of these instruments deepens the knowledge that can be gained and generated from surveying communities in the context of disasters, diversifies knowledge generation, and informs survey design and deployment in ways that hold the potential to inform both public health practice and theory. By bringing together academic and community experts, this allowed the survey to not diverge from community priorities and confirmed the usability of such a tool for people outside of academia. Comprehensive assessment tools are crucial for understanding the diverse health needs of the community, collecting data on food, water, energy security, chronic conditions, disabilities, and mental health indicators. This survey can help anticipate and address these needs, ultimately mitigating the effects of hazards, and facilitate coordinated responses among individuals, households, community leaders, and aid organizations, such as local or state health departments, government agencies, and non-governmental organizations.
The co-development of this survey has several significant public health implications for underserved communities that rely on self-management for emergency preparedness and disaster response. First, this survey can help identify at-risk populations and address social-ecological or technical vulnerabilities across mitigation, preparedness, response and/or recovery. Second, this survey can aid in proper allocation of resources (e.g., respond to lack of access to clean water, mental health in the community, need of electricity for energy dependent equipment). Third, this survey can be utilized to monitor health outcomes, such as Public health officials and community leaders evaluating and using data for interventions in the community. Fourth, data collection can inform evidence-based policy by highlighting social determinants of health and health disparities within a community for resource advocacy, coordination and cross-sector collaboration (i.e., residents, public health officials and emergency managers). Overall, the co-development of this survey provides a comprehensive understanding of community needs and assets to address the complexities of disasters.
Future Research Directions
Our future research will involve continuing efforts to validate the pilot survey with academic and community experts and incorporating the feedback into refining the pilot survey (Figure 1). We aim to consider the useability of the protocol after a hazard event in Corcovada in the future and will develop ways in which to improve its uptake and use, as necessary. Third, we will begin steps to adapt and recontextualize the survey instrument for other municipalities and townships in Puerto Rico. The Project Team will seek external funding for this activity. The ultimate objective is to develop a standardized survey template that can be adapted as required, iteratively over time or in different contexts, by communities without significant investments. To be more specific, the survey instrument can support different communities in developing not only mitigation and preparedness plans, but also in applying for hazard mitigation grant programs for community capacity-building programs.
Acknowledgements. We extend our gratitude to the community leaders and residents of Corcovada, Puerto Rico, for their time and invaluable contributions to this collaboration. We also would like to thank Javier Nieves Torres for their support in the validation of our “before hazard” survey and Ryelie Barnes for her support with our project toolkit and website.
References
-
Zscheischler, J., Westra, S., Hurk, van den Hurk, B. J. J. M., Seneviratne, S. I., Ward, P. J., Pitman, A., AghaKouchak, A., Bresch, D. N., Leonard, M., Wahl, T., & Zhang, X. (2018). Future climate risk from compound events. Nature Climate Change, 1–9. http://doi.org/10.1038/s41558-018-0156-3 ↩
-
Zscheischler, J., Martius, O., Westra, S., Bevacqua, E., Raymond, C., Horton, R. M., van den Hurk, B., AghaKouchak, A., Jézéquel, A., Mahecha, M. D., Maruam, D., Ramos, A. M., Ridder, N. N., Thiery, W., & Vignotte, E. (2020). A typology of compound weather and climate events. Nature Reviews Earth & Environment, 1–15. http://doi.org/10.1038/s43017-020-0060-z ↩
-
Thomas, D. S. K., Jang, S., & Scandlyn, J. (2020). The CHASMS conceptual model of cascading disasters and social vulnerability: The COVID-19 case example. International Journal of Disaster Risk Reduction, 51, 101828. http://doi.org/10.1016/j.ijdrr.2020.101828 ↩
-
Intergovernmental Panel on Climate Change. (2021). Summary for Policymakers. Climate Change 2021: The physical science basis. Contribution of Working Group I to the Sixth Assessment Report of the Intergovernmental Panel on Climate Change. https://www.ipcc.ch/report/ar6/wg1/downloads/report/IPCC_AR6_WGI_SPM.pdf ↩
-
Roque, A., Shah, S., Tormos-Aponte, F., & Quintana Torres, E. (2022). Social Capital, Community Health Resilience, and Compounding Hazards in Corcovada, Puerto Rico. Natural Hazards Center Public Health Report Series, 16. University of Colorado Boulder. https://hazards.colorado.edu/public-health-disaster-research/social-capital-community-health-resilienceand-compounding-hazards-in-corcovada-puerto-rico ↩
-
Dargin, J., Berk, A., & Mostafavi, A. (2020). Assessment of household-level food-energy-water nexus vulnerability during disasters. Sustainable Cities and Society, 62, 102366. ↩
-
Wells, E. M., Boden, M., Tseytlin, I., & Linkov, I. (2022). Modeling critical infrastructure resilience under compounding threats: a systematic literature review. Progress in Disaster Science, 100244. ↩
-
Ashby, S., Kleve, S., McKechnie, R., & Palermo, C. (2016). Measurement of the Dimensions of Food Insecurity in Developed Countries: A Systematic Literature Review. Public Health Nutrition, 19(16), 2887-2896. ↩
-
Eicher-Miller, H. A., Mason, A. C., Weaver, C. M., McCabe, G. P., & Boushey, C. J. (2009). Food insecurity is associated with iron deficiency anemia in US adolescents. The American Journal of Clinical Nutrition, 90(5), 1358-1371. ↩
-
Wutich, A., & Ragsdale, K. (2008). Water insecurity and emotional distress: coping with supply, access, and seasonal variability of water in a Bolivian squatter settlement. Social Science & Medicine, 67(12), 2116-2125. ↩
-
Sultana, F. (2011). Suffering for water, suffering from water: Emotional geographies of resource access, control and conflict. Geoforum, 42(2), 163-172. ↩
-
Wutich, A., Brewis, A., & Tsai, A. (2020). Water and mental health. Wiley Interdisciplinary Reviews: Water, 7(5), e1461. ↩
-
Brewis, A., Roba, K. T., Wutich, A., Manning, M., & Yousuf, J. (2021). Household water insecurity and psychological distress in Eastern Ethiopia: Unfairness and water sharing as undertheorized factors. SSM-Mental Health, 1, 100008. ↩
-
Rosinger, A. Y. (2018). Household water insecurity after a historic flood: Diarrhea and dehydration in the Bolivian Amazon. Social Science & Medicine, 197, 192-202. ↩
-
Rosinger, A. Y., & Young, S. L. (2020). The toll of household water insecurity on health and human biology: current understandings and future directions. Wiley Interdisciplinary Reviews: Water, 7(6), e1468. ↩
-
Stoler, J., Miller, J. D., Brewis, A., Freeman, M. C., Harris, L. M., Jepson, W., ... & Tutu, R. (2021). Household water insecurity will complicate the ongoing COVID-19 response: evidence from 29 sites in 23 low-and middle-income countries. International Journal of Hygiene and Environmental Health, 234, 113715. ↩
-
Hernández, D. (2013). Energy insecurity: a framework for understanding energy, the built environment, and health among vulnerable populations in the context of climate change. American Journal of Public Health, 103(4), e32-e34. ↩
-
Lopez-Cardalda, G., Lugo-Alvarez, M., Mendez-Santacruz, S., Rivera, E. O., & Bezares, E. A. (2018, October 23-24). Learnings of the complete power grid destruction in Puerto Rico by Hurricane Maria [Conference presentation paper]. 2018 IEEE International Symposium on Technologies for Homeland Security, Woburn, MA, United States. https://ieeexplore.ieee.org/document/8574120 ↩
-
Clay, L. (2022). Post-Disaster Food & Nutrition Security: The Disaster Food Security Framework (DFSF). Innovation Brief. Local and Regional Food Systems Response to COVID: Recovery and Resilience. https://lfscovid.localfoodeconomics.com/wp-content/uploads/2023/03/DisasterFoodSecurityFramework.pdf ↩
-
Daher, B., Hamie, S., Pappas, K., Nahidul Karim, M., & Thomas, T. (2021). Toward resilient water-energy-food systems under shocks: Understanding the impact of migration, pandemics, and natural disasters. Sustainability, 13(16), 9402. ↩
-
Schmidt, J. I., Johnson, B., Huntington, H. P., & Whitney, E. (2022). A framework for assessing food-energy-water security: A FEW case studies from rural Alaska. Science of The Total Environment, 821, 153355. ↩
-
U.S. Department of Agriculture. (2012, September). Household Food Security Survey Module: Three-stage design, with screeners. Economic Research Service. https://www.ers.usda.gov/media/8271/hh2012.pdf ↩
-
Young, S. L., Boateng, G. O., Jamaluddine, Z., Miller, J. D., Frongillo, E. A., Neilands, T. B., ... & Stoler, J. (2019). The Household Water InSecurity Experiences (HWISE) Scale: development and validation of a household water insecurity measure for low-income and middle-income countries. BMJ Global Health, 4(5), e001750. ↩
-
Botman S., Moore, T.F., Moriarity, C.L., & Parsons, V.L. (2000). Design and estimation for the National Health Interview Survey, 1995–2004. National Center for Health Statistics. Vital Health Stat 2(130). ↩
-
Cook, J. T., Frank, D. A., Casey, P. H., Rose-Jacobs, R., Black, M. M., Chilton, M., de Cuba, S. E., Appugliese, D., Coleman, S., Heeren, T., Berkowitz, C., & Cutts, D. B. (2008). A brief indicator of household energy security: associations with food security, child health, and child development in US infants and toddlers. Pediatrics, 122(4), e867-e875. ↩
-
Colton, R. D., Fisher, S., Finance, C. P., Economics, G., & Belmont, M. A. (2008). Public Health Outcomes Associated with Energy Poverty: An Analysis of 2007 Iowa Behavioral Risk Factor Surveillance System (BRFSS) Data from Iowa. Iowa Department of Human Rights, Bureau of Energy Assistance. https://www.fsconline.com/downloads/Papers/2008%2006%20Iowa_BRFSS-final.pdf ↩
-
Boateng, G. O., Balogun, M. R., Dada, F. O., & Armah, F. A. (2020). Household energy insecurity: dimensions and consequences for women, infants and children in low-and middle-income countries. Social Science & Medicine, 258, 113068. ↩
-
Brewis, A., Workman, C., Wutich, A., Jepson, W., Young, S., & Household Water Insecurity Experiences–Research Coordination Network (HWISE‐RCN) (2020). Household water insecurity is strongly associated with food insecurity: Evidence from 27 sites in low‐and middle‐income countries. American Journal of Human Biology, 32(1), e23309. ↩
-
Centers for Disease Control and Prevention. (2019). Community Assessment for Public Health Emergency Response (CASPER) Toolkit (3rd ed.). https://www.cdc.gov/nceh/casper/docs/CASPER-toolkit-3_508.pdf ↩
-
Schnall, A., Nakata, N., Talbert, T., Bayleyegn, T., Martinez, D., & Wolkin, A. (2017). Community Assessment for Public Health Emergency Response (CASPER): an innovative emergency management tool in the United States. American Journal of Public Health, 107(S2), S186-S192. ↩
-
McDavid, K., & Cruz, M. (2019). Environmental health shelter assessments: Using tools to protect occupants after disasters. Journal of Environmental Health, 82(5), 32-34. ↩
-
Noe, R. S. (2018). Applications: Disaster-related mortality surveillance: Challenges and considerations for local and state health departments. In J.A. Horney (Ed.), Disaster Epidemiology (pp. 55-63). Academic Press. https://www.sciencedirect.com/science/article/abs/pii/B9780128093184000071 ↩
-
Lillibridge, S. R., Noji, E. K., & Burkle Jr, F. M. (1993). Disaster assessment: the emergency health evaluation of a population affected by a disaster. Annals of Emergency Medicine, 22(11), 1715-1720. ↩
-
Roque, A., Wutich, A., Brewis, A., Beresford, M., García-Quijano, C., Lloréns, H., & Jepson, W. (2021). Autogestión and water sharing networks in Puerto Rico after Hurricane María. Water International, 46(6), 938-955. ↩
-
Vega, K. S. (2019). Puerto Rico weathers the storm: Autogestión as a coalitional counter-praxis of survival. Feral Feminisms, 9, 39-55. ↩
-
Mulligan, J. M., & Garriga-López, A. (2021). Forging compromiso after the storm: activism as ethics of care among health care workers in Puerto Rico. Critical Public Health, 31(2), 214-225. ↩
-
Kelley, A., Piccione, C., Fisher, A., Matt, K., Andreini, M., & Bingham, D. (2019). Survey Development: Community Involvement in the Design and Implementation Process. Journal of Public Health Management and Practice, 25(5), S77–83. http://doi.org/10.1097/PHH.0000000000001016 ↩
-
Asencio-Yace, J. I. (2020). Sustainable community aqueducts as models for community microgrids: an in-depth case study of Corcovada Arriba's governance and management practices [Thesis, Universidad de Puerto Rico Mayagüez]. UPR Recinto de Mayagüez. https://scholar.uprm.edu/entities/publication/28823ea9-4fbd-4be8-9f90-2445bbd08fba ↩
-
Chandra, A., Marsh, T., Madrigano, J., Simmons, M. M., Abir, M., Chan, E. W., Ryan, J., Nanda, N. Ziegler, M.D., & Nelson, C. (2021). Health and social services in Puerto Rico before and after Hurricane Maria: Predisaster conditions, hurricane damage, and themes for recovery. Rand Health Quarterly, 9(2). ↩
Roque, A. D., Quintana Torres, E., Shah, S. H., Painter, M. P., Cuevas, F., & Tormos-Aponte, F. (2023). Assessing Intra-Community Public Health Impacts from Compounding Food, Energy, and Water Insecurities (Natural Hazards Center Public Health Disaster Research Report Series, Report 37). Natural Hazards Center, University of Colorado Boulder. https://hazards.colorado.edu/public-health-disaster-research/assessing-intra-community-public-health-impacts-from-compounding-food-energy-and-water-insecurities