 In September 2005, I was deployed to Nigeria as a clinical psychologist by Medicines Sans Frontiers/Doctors Without Borders (MSF). The emergency response followed a series of outbreaks of violence in the central Nigerian state of Plateau. In early May 2004 thousands of Nigerians fled from central Plateau State after clashes between rival militia culminated in a series of massacres. In the immediate aftermath of this horrendous tragedy, MSF created mobile clinics to medically assist more than 10,000 displaced people living in makeshift camps under extremely difficult conditions.
In September 2005, I was deployed to Nigeria as a clinical psychologist by Medicines Sans Frontiers/Doctors Without Borders (MSF). The emergency response followed a series of outbreaks of violence in the central Nigerian state of Plateau. In early May 2004 thousands of Nigerians fled from central Plateau State after clashes between rival militia culminated in a series of massacres. In the immediate aftermath of this horrendous tragedy, MSF created mobile clinics to medically assist more than 10,000 displaced people living in makeshift camps under extremely difficult conditions.
Two particularly brutal attacks took place in Yelwa, a market town located in the southern part of Plateau State. On February 4, 2004, armed Muslims killed more than 75 Christians and in an act of retaliation, on May 2 and 3, large numbers of armed Christians surrounded Yelwa, and killed more than 700 Muslims. Much of the city was destroyed and thousands of people were displaced.
MSF provided emergency medical aid to those who had fled Yelwa and helped with reintegration efforts once the violence had subsided. While treating many physically injured adults and children in displaced persons camps, members of the MSF team began hearing the horrific stories of what people had experienced during the attacks. The team realized that many survivors, including children, were experiencing acute trauma responses, including numbing, emotional detachment, muteness, depersonalization, psychogenic amnesia. They also had continued re-experiencing of the event via thoughts, dreams and flashbacks, as well as avoidance of any stimulation that reminded them of the event. MSF recruited me to help launch a psychosocial program aimed at helping adults and children as they returned home and tried to rebuild their shattered lives. The program we created for traumatized children used creative techniques and community support to achieve its success.
We learned much from developing and implementing this program. Prior to this I had only used art therapy in the United States with adults and children who have either survived a traumatic event or were coping with a traumatic loss. What we designed became the first of many projects in which I integrated art therapy to help people recover from trauma in disaster contexts globally. The events that occurred in this village in Nigeria changed my life, and showed me the power of art therapy to help heal seemingly unbearable trauma among survivors of heinous crimes. During my tenure in Yelwa MSF provided art therapy and counseling to approximately 2,500 children enrolled in schools in Yelwa and the surrounding area. The story that follows summarizes how our work helped trauma victims and became a catalyst for future integrative projects.

(L) Church in Yelwa, where at least 48 Christians were killed on February 24, 2004 (R) Central mosque, Yelwa, destroyed during the May 2004 attack © Human Rights Watch
Arriving
Among the first things I saw when driving into Yelwa in our white Land Cruiser were crumbled buildings and mass grave sites, eerie reminders of the brutal attacks that had occured just a year prior to my arrival. After the attacks market life was initially scarce in Yelwa and in the surrounding towns of Garkaka and Longvel. A pulse gradually returned to these previously lively towns and when I arrived street life was back in full swing.
The vendors weren’t the only people who had dissappeared from the streets in the aftermath of the attacks. My colleagues informed me that there was a noticible absence of police and military, something that many people viewed with suspicion. Once a military presence returned roadblocks became commonplace on the roads into Yelwa. At first, MSF gave out condoms—a coveted commodity in a country where HIV is rampant—as a way to quickly pass through the road blocks. We quickly learned however, that this practice was affecting others who were also trying to pass through the roadblocks as they had nothing to give (see text box page 16).
Getting Started
When it comes to mental health services following man-made disasters, building relationships and trust is an obligation, not an option. Therefore, we quickly determined that the local team of counselors selected from the community and trained on basic mental health skills would need to represent both sides of the conflict—men and women, Christians and Muslims. After a rather large round of interviews, which included role play, a team of five local counselors were selected. I became their clinical supervisor and trainer. The first round of intensive training lasted one month. All of the new counselors had experienced the violence first hand, meaning they were both survivors and providers, and they often needed additional support to work through their own trauma experiences tied to the crisis. The material processed in group supervision mirrored the issues faced in the community. For example, issues related to trust between the Christian and Muslim counselors played out right there in our supervision meetings and the counselors were able to process and make meaning of this experience both as professionals as well as members of their respective communities. This helped them facilitate their trauma groups and work with community members from different groups and see issues from multiple perspectives.
Together we examined stereotypes and biases and team dynamics improved as authentic relationships were formed and maintained. That decision to have a representative team was a game-changer. The diverse team of psychosocial counselors quickly became known as the “Fab Five.” As the trust among team members grew, so did the numbers of referrals we received to our support groups and school-based art therapy programs. Within a few months we had a wait list for services and I was given approval to hire an additional counselor. The team was subsequently referred to as “Fab Five Plus One.” They were respected and consulted frequently because they could diplomatically update the international staff on the nuances of the conflict in a matter of minutes and help us get the root cause of any social, cultural, or governmental roadblock put in our way.
Project Structure
Psychoeducation
In the treatment literature, much attention is paid to the cognitive and emotional processing of traumatic memories (Briere, 2003; Allen, 1991; Flack, Litz, & Keane, 1998; Friedman, 2000a; Najavits, 2002). Nevertheless, psycho-education is also an important aspect of the early stages of trauma recovery. Many survivors of interpersonal violence were victimized in the context of an established relationship to their perpetrator or in this case, perpetrators. As a result, the traumatic experience is difficult to make sense of; and, in the case of children, it occurs at a relatively early stage of cognitive development. This lack of cognitive development impairs their ability to accurately and coherently understand what has happened.
Child survivors often carry fragmented, incomplete, or inaccurate explanations of traumatic events into adulthood, with predictable negative results. Psychoeducational activities are therefore helpful in the therapy process. As the client addresses traumatic material, he or she may gain from additional information that normalizes or provides a new perspective on their traumatic memory. Our local Nigerian psychosocial counselors assisted in this area by providing accurate information to their clients on the nature of trauma and its effects on both the survivor as well as on his or her support system.
Children are one of the most under-served populations among disaster survivors. When it comes to assessing their needs in a post-conflict or post-disaster setting, children’s capacity for resilience is often overstated by the adults and other care-givers around them. This is due to a misunderstanding of why children engage in play. Statements such as “he’s already playing again, he’s going to be just fine,” can be dangerous and misleading. I once watched a young girl practice calling 911 over and over again while “playing” with a large doll house. During therapy, I learned she blamed herself for her mother’s death because she believed she did not call for help early enough. This had not been discovered during the initial interviews because this young girl was dissociated and highly emotionally regulated. For all intents and purposes, she looked to be coping just “fine.” What appeared to be resilience and control was actually a masking of much deeper fears and regrets.
Disasters can have far reaching and long-lasting effects on the mental health of a child. Some children can appear “just fine” in the immediate aftermath, only to suffer greatly down the road with all sorts of issues, including sleeping problems, trust and intimacy issues, emotional regulation, frustration tolerance, and self-soothing deficits. Art therapy in the immediate aftermath of disaster has been demonstrated—by the team in Yelwa and many other scenarios-- to be effective in reducing these impacts on children (Roje 1995, Orr, 2007, Chilicote 2007, Howie et. al 2002).
Project Launch
The MSF mental health team first visited schools and community leaders in Yelwa to explain how children might manifest their trauma. Difficulty concentrating, crying jags, becoming easily upset in the classroom, missing school, poor academic performance and/or substance use were frequently reported. Once educated about the impact of trauma and trauma responses, the teachers in Yelwa felt empowered by new information and could make sense of what appeared to be senseless behavior. Their attitudes changed, their frustrations decreased and they quickly became our best referral source. Taking time to educate the teacher about trauma was a way to offer them support.
Clinical Programming
In group or individual sessions, participating children learned how their feelings and behaviors were linked to their personal experiences. MSF counselors used drama, drawings, breathing techniques, and most of all, talking and listening. Regularly talking and listening to others helped participants put their own problems in perspective. They learned that while many children were struggling to make sense of what happened, few were speaking openly about it. They also realized they were not the only ones struggling, and they were relieved to hear others discuss what they were experiencing. This exchange among children helped to reduce the obvious (conduct disordered) problematic behavior and the not-so-obvious (dissociated, shut down) behavior teachers were seeing in the classroom and family members were seeing at home. Both the obvious and less obvious behaviors are important to note because sometimes it is only the children who are “acting out” that are identified for help. Children who are shut down should also be assessed and supported.
The art-based intervention that was developed for this project lasted six sessions and included pre- and post interviews of the participants who ranged in age from 6 to 18. Both Muslims and Christian children took part. At the end of the intervention, they evaluated the local counselors. During the course of the intervention the MSF psychosocial team focused on the following topics: establishing safety, remembrance and mourning, bridging life before and after the traumatic event, and exploring the children’s hopes and dreams for the future. Along with a semi-structured discussion, the MSF psychosocial counselors distributed paper and pens and created a safe space so that the children could freely draw a picture that aligned with the topic under discussion.
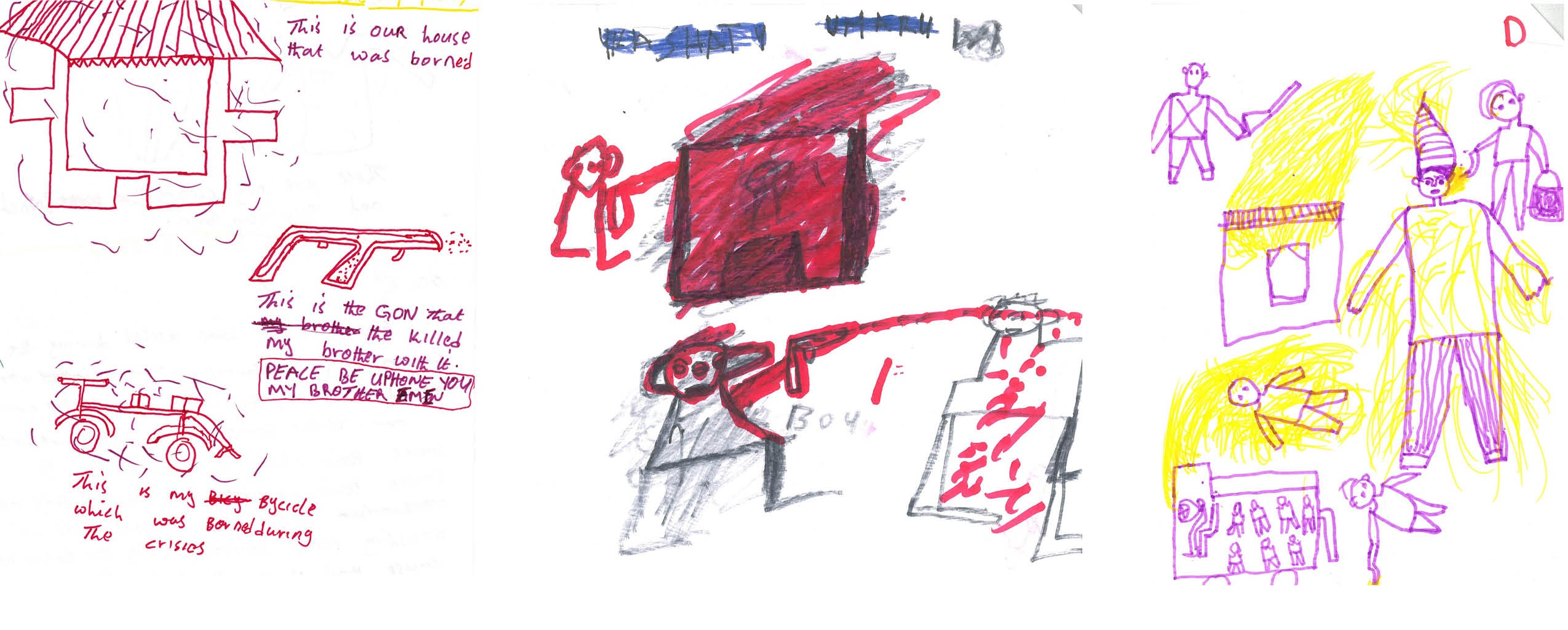
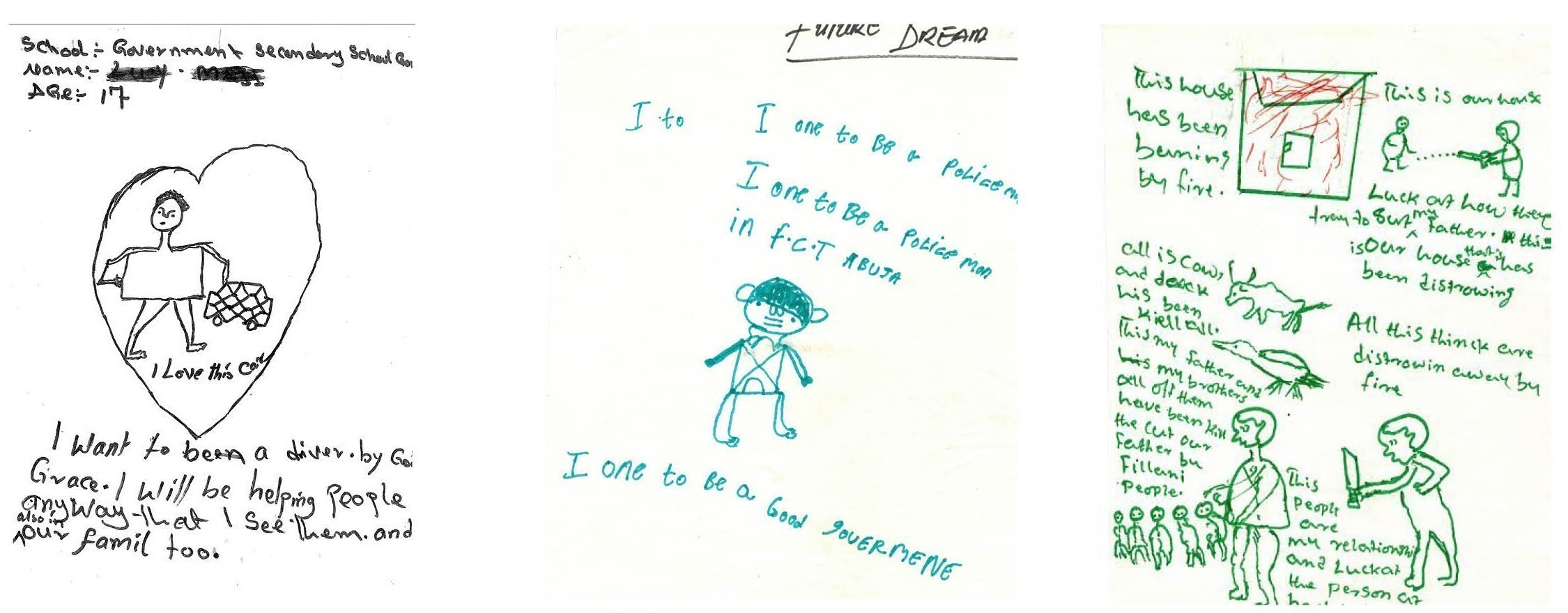
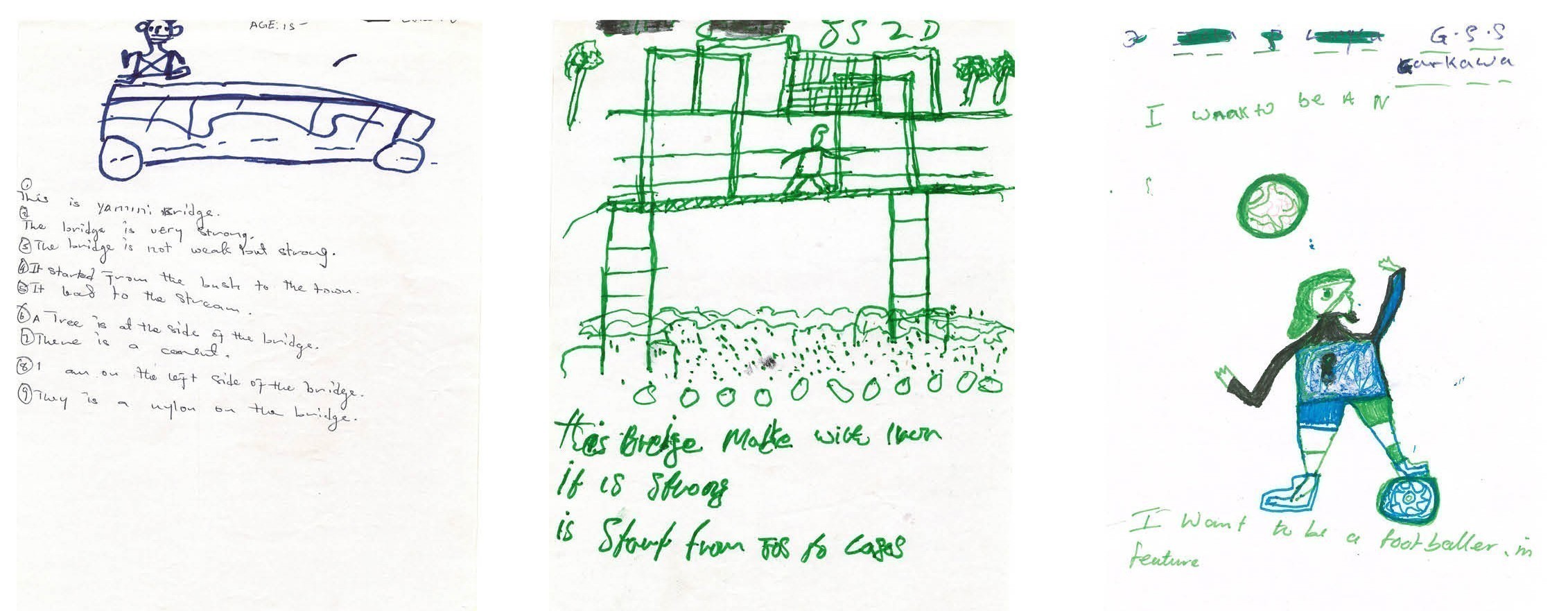
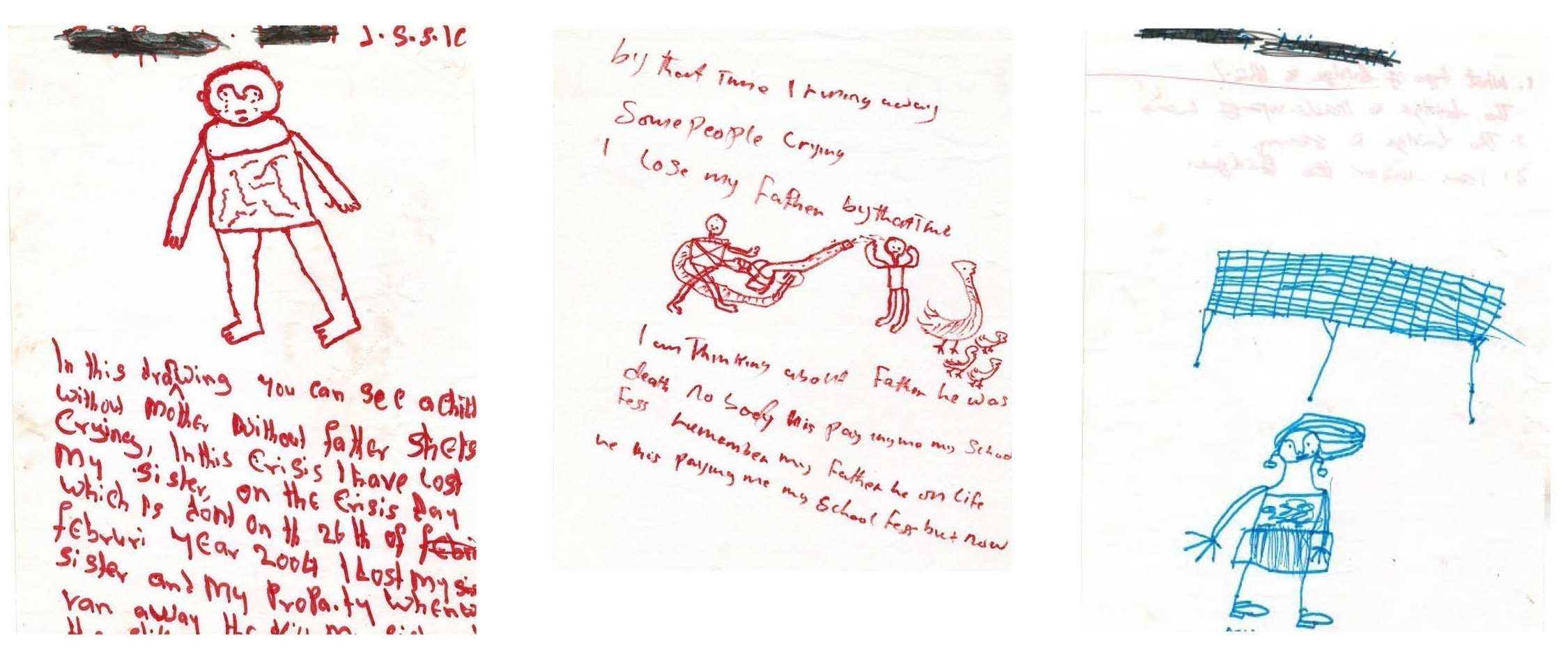
In the first weeks the youngsters bent over their pieces of paper, concentrating intensely as horrific scenes took shape: men with oversized weapons, people riddled with bullets, burning houses, and people with severed limbs. One boy even captured on paper what had happened at the local soccer field: a heinous event where three young men from the community were brutally murdered on the field. This drawing sheds light on the bizarre avoidance and resistance many teachers and parents were seeing from their children when encouraged to “just go play futbal.” Later on, the students focused on drawing elaborate bridges. The bridge symbolizes an individual’s perception of the world (dangerous or safe) and of his or her control over the environment (low or high). Each participant was asked to draw a bridge and place him or herself in the picture. They also drew soccer stars and medical doctors, capturing their dreams for the future and how they might achieve them.
During the different activities, the local counselors asked the children to explain their drawings and listened to the descriptions: father shot, uncle decapitated, sister abducted, house ransacked and burned down, sharks under the shaky bridge to safety, dreams of becoming a teacher. The children recounted hundreds of traumatic scenes in uncannily absent, seemingly calm voices. The transition activities were important to help the children put space and time between the traumatic events and where they hoped to be. In the dream sequence many of the children laughed and acted playful.
Over the course of my time in Yelwa, it became clear that some children strained to express their emotions and traumatic memories verbally, but on paper, where anything was fair game, they vividly, graphically, shared their experiences in drawings. The pictures they drew captured what worried, scared, and motivated them.
Mobile Art Exhibit
At the end of the six-week intervention, the children were asked what they wanted to do with their pictures. A few of them wanted to burn or bury the more painful renderings, as a way to mourn or move past what they had experienced or lost. The local counselors offered some clients a grieving ceremony, in which they buried a picture or arranged for a symbolic funeral ceremony with family for a lost loved one. They often sang local funeral songs and reminisced about the person the child had lost. Other kids asked if their art could be exhibited for their families and communities to see. The clinical psychologist who values privacy above all else in me baulked at the idea of publicizing what was confidential therapeutic material. But the social justice advocate in me learned that by allowing these children to exhibit their artwork we were giving them a platform to be seen and valued as artists and members of the community. The experience of exhibiting their work helped the children feel empowered as they were treated as artists who had accomplished something, rather than as victims or clients.
The communities in Yelwa came out in droves and the country office in Abuja, 2,000 miles away, also held a series of incredibly well attended events to further highlight the program and allow for the pictures to be seen. Many of the children showed signs of post-traumatic growth, or a positive change experienced as a result of the struggle with a major life crisis or a traumatic event. Further, they showed up to the mobile art exhibits in their best clothes with large smiles on their faces. The talked about feeling more secure and their behavior in school and at home underlined this perception of growth.
This art therapy project was successful in helping these children break free of elements of their traumatic experiences. By simply having a safe place to tell and draw their stories, the children were able to integrate horrific experiences into their lives. Most of the kids improved in multiple areas of functioning--as evidenced by improved performance in school and better relationships with friends and family. Since the conclusion of this project I have integrated the arts—both drawing and photography—into recovery efforts around the world, including in Northern Thailand with Shan Migrants, and in Liberia with torture survivors.
Thanks to modern social media, namely Facebook, I have reconnected with three of the six “Fab Five Plus One” over the last two years. One, tragically, died from AIDS. The other two are reportedly living happy lives with their families. Unfortunately, they are no longer working as psychosocial counselors; their lives quickly converted back to the ones they were leading before MSF came to town and hired and trained them. The lack of local organizational capacity building and hand-off to local partners is one area of disaster response and development that could use more work. Integrating ideas about sustainability can be hard when developing a disaster response, but is essential if an organization wants to have a lasting impact. Far too many times, good projects end when the seed funding runs out and no plan for sustainability has been created.
One of the women I connected with went back to teaching and has a small pharmacy. The other went back to school and secured a government position in the capital of the Plateau State.
In the Plateau region things haven’t changed much, although no violent outbursts have occurred since the 2004 attacks. Both team members note the tensions between Muslims and Christians in their correspondence, but they do not feel directly affected by these tensions and are leading stable peaceful lives.
I am grateful that I am able to stay connected to these wonderful people. I deeply enjoy reminiscing with them. I smile when they remind me of things I would say wrong in Housa, their local language, such as “my bag is inside the donkey” when attempting to say “my bag is inside the car.” They continue to deeply affect me, both professionally and personally, and I will be forever impressed by and grateful for the work they did in the aftermath of this horrific man-made disaster.
Background
Since the 2014 kidnapping of the Chibok schoolgirls by Boko Haram, a branch of the Islamic State of Iraq that has been active since 2009, Nigeria has been in the news a lot (Human Rights Watch 2005). But religious-related violence predates the emergence of Boko Haram. Africa’s most populous nation, with 150 million people, has seen a steady rise in violence between the Muslim north and Christian south of the country since its independence in 1960. Nevertheless the roots of the violence go beyond religion.
The 2004 conflict in Plateau State, for example, stems from longstanding disputes over land, political, and economic privileges between ethnic groups who consider themselves original inhabitants of a particular area, called indigenes, and those whom they view as settlers. Until 2001 these disputes had never led to large-scale loss of life, but in September of that year, tensions suddenly exploded in Jos, the state capital, and around 1,000 people were killed in just six days. What had started as a political conflict turned into a religious one as the ethnic divide happened to coincide with the religious divide. The tensions between indigenes and settlers became a conflict between Christians and Muslims, as both sides used religion as a rallying cry to drag other groups into the conflict. After the attacks in Jos, the violence soon spread out to other parts of the Plateau State. In the years to follow poverty and regional oppression further fueled the fire.
Despite the escalation of the conflict in this area since September 2001, and clear warning signs of the likelihood of further violence, the Nigerian government did not take any effective action and allowed the conflict to spiral out of control. Finally when Yelwa was attacked on May 2 and 3, 2004, the scale of the violence could no longer be ignored. On May 18, Nigerian President Olusegun Obasanjo declared a state of emergency in Plateau State (Human Rights Watch 2005).
References
Allen, J. G. (2005). Coping with trauma: Hope through understanding. Washington, DC: American Psychiatric Press. Briere, J. (2003). Integrating HIV/AIDS prevention activities into psychotherapy for child sexual abuse survivors. In L. Koenig, A. O’Leary, L. Doll, & W. Pequenat (Eds), From child sexual abuse to adult sexual risk: Trauma, revictimization, and intervention (pp. 219–232). Washington, DC: American Psychological Association. Chilcote, R. L. (2007). "Art Therapy with Child Tsunami Survivors in Sri Lanka". Art Therapy: Journal Of The American Art Therapy Association, 24(4), 156-162. Herman, J. L. (1992). Trauma and recovery: The aftermath of violence—from domestic abuse to political terror. New York: Basic Books. Howie, P., Burch, B., Conrad, S., & Shambaugh, S. (2002). "Releasing trapped images: Children grapple with the reality of the September 11 attacks". Art Therapy, 19(3), 100-105. Human Rights Watch. (2005, May). "Revenge in the Name of Religion: The Cycle of Violence in Plateau and Kano States". Vol. 17, No. 8 (A). http://www.hrw.org/reports/2005/nigeria0505/nigeria0505.pdf, (accessed on June 15, 2015). Najavits, L. M. (2002). Seeking safety: A treatment manual for PTSD and substance abuse. New York: Guilford. Orr, P. P. (2007). "Art therapy with children after a disaster: A content analysis". The Arts In Psychotherapy, 34(4), 350-361. Resick, P. A., & Schnicke, M. K. (1993). Cognitive processing therapy for rape victims: A treatment manual. Newbury Park: Sage. Roje, J. (1995). "LA 94 earthquake in the eyes of children: Art therapy with elementary school children who were victims of disaster". Art Therapy, 12(4), 237-243.
Mitchell has worked for many years as a trauma psychologist for humanitarian organizations including Doctors without Borders and the Center for Victims of Torture in various locations including Nigeria, Liberia, South Africa, Sierra Leone, Jordan, Myanmar, Thailand and Bosnia. She has particular interest in staff welfare, capacity building, refugee mental health and interpersonal violence. She has also provided support for humanitarian staff and was a member of a UNICEF technical work group focused on child protection inside Myanmar. Mitchell played a part in the development of a mental health policy for the country of Liberia and has developed programming for marginalized groups including people living with HIV/AIDS, LGBTQ communities, former political prisoners and torture survivors.
Mitchell has authored and co-authored various publications in the areas of: Post Traumatic Stress Disorder (PTSD) in refugees, Post Traumatic Growth (PTG), counseling applications with people of African ancestry, the impact of war on civilians, therapeutic photography, group interventions with vulnerable populations in Myanmar, re-entry trauma and the experience of working as a psychologist internationally.