Stress During Pregnancy Due to a Natural Disaster in Vanuatu: Effects on Infant Development in a Low-Middle Income Country
Kelsey Needham Dancause
Université du Québec à Montréal
Alysa Pomer
Binghamton University
Publication Date: 2015
Overview
Psychosocial stress during pregnancy affects not only the mother, but also her child. At high levels, maternal stress hormones can cross the placenta and affect fetal development1. Prenatal stress has been associated with poor adverse birth outcomes2, such as smaller birth length3 4 5, weight3 5 6, and gestational age3 4 5; low birthweight7 8; and preterm birth7 8 9 10. Natural disasters provide excellent models of prenatal stress because the stressor is independent of maternal and household traits that might also affect infant growth11. However, these studies are difficult to design because we must act quicky after the disaster to create and distribute the surveys if we are to obtain reliable indices of stress.
In 2015, the Republic of Vanuatu, a low-middle income country in the South Pacific, experienced a major cyclone that left many villages in ruins. Building on our past experience analyzing population health in Vanuatu12 13 14 15 16, and analyzing prenatal stress in other settings following natural disasters4 17 18, we sought to create a study of prenatal stress following a natural disaster in Vanuatu.
Our primary research question in this round of data collection was: What was the degree of hardship, distress, and dietary change among adult women in Vanuatu due to Cyclone Pam? Do patterns differ among pregnant and non-pregnant women?
The data collected after the disaster with support from the Natural Hazards Center provides the baseline for analyzing relationships between hardship, distress, and nutritional change due to the cyclone, and the health outcomes of infants who were in utero during the cyclone.
Methods
We created a self-report survey to assess maternal demographics (age, number of children, area of residence); hardship and distress due to the cyclone; and nutritional patterns following the cyclone. Women of reproductive age on four islands (Aneityum, Efate, Erromango, and Tanna) were invited to participate.
The final survey packet is attached with the report. Surveys were translated into Bislama, the local language, by K Dancause and colleagues at the Vanuatu Ministry of Health, and reviewed by health officials and local residents before distribution.
Objective Hardship was assessed using a custom-made survey of experiences during and following the cyclone, based on those already created and used in three other studies of prenatal stress in which K Dancause has participated: Project Ice Storm (Canada), the Iowa Flood Study (USA), and the Queensland Flood Study (Australia)11: . The surveys are created to measure four aspects of hardship following a disaster: Threat, Loss, Scope, and Change. The measure in Vanuatu was an adaptation specific to the country and to the disaster. We assessed damage to the village, house, and garden; loss of livestock; loss of personal items; accessability of food and water after the cyclone; women’s perceptions of their current access to food, water, and housing; and the degree to which their lives had returned to the way they were before the cyclone.
Subjective Distress was assessed using a Bislama adaptation of the Impact of Events Scale – Revised19, the questionnaire commonly used to assess symptoms of post-traumatic stress disorder. All questions were translated into Bislama, reviewed by health officials and local residents, and then questions that were redundant following translation were trimmed. Women reported on a scale of 0 (“not at all”) to 4 (“all the time”) the extent to which they experienced symptoms in three categories of distress – hyperarousal, avoidance, and intrusive thoughts – relative to the cyclone.
Nutritional patterns were assessed using 24-hour dietary recall in which women were instructed to write everything they had eaten in the morning, afternoon, and night the previous day; and a food frequency questionnaire asking women how many times in the past week they had eaten food from 15 different categories.
Upcoming Data Collection
Birth Records: Following the expected delivery dates of all pregnant women in the sample, we will return to Vanuatu to scan birth records routinely collected by the Vanuatu Ministry of Health. These include mothers’ names and location of residence as identifiers, complications with the pregnancy (maternal illnesses, etc.), and infants’ characteristics at birth (gestational age, birth weight, birth length, head circumference, etc.) Data for women who provided consent for us to access medical records will be entered into a database to allow us to analyze relationships among hardship and distress due to the cyclone, and health outcomes of the pregnancy and the infant.
General psychosocial health: At the time of the collection of birth records, we will begin the collection of data on general psychosocial health measures among pregnant women, including the State-Trait Anxiety Inventory20, Perceived Stress Scale21, Pregnancy Experience Scale22, and the Edinburgh Postnatal Depression Scale23. Collecting these data one year after the cyclone will help to ensure that women’s responses are not biased by the distress associated with the cyclone. Together with the data on hardship and distress from the cyclone, and data on birth outcomes, the complete dataset and will allow us to analyze the effects of both acute and chronic stress during pregnancy on infant outcomes in Vanuatu.
Preliminary Analyses
Our preliminary analyses have focused on maternal distress. We used one-way ANOVA to test differences in demographic variables among pregnant and non-pregnant women. We used Pearson correlations to test relationships among distress and maternal demographic variables. We used one-way ANOVA to test differences in mean distress levels among pregnant and non-pregnant women, and among islands. Finally, we used General Linear Models to test differences in distress levels among pregnant and non-pregnant women controlling for island of residence and demographic characteristics. Statistical significance was defined as p<0.05. Analyses were conducted with SPSS version 22 (IBM Statistics).
For a subset of women whose objective hardship data have been finalized, we tested relationships among two measures of objective hardship – damage to the village and damage to the home – with subjective distress due to the cyclone using Pearson correlations.
Results of Preliminary Analyses
We collected demographic, stress, and nutritional surveys for 800 women on five islands affected to varying degrees by the cyclone. Of these, 184 were pregnant at the time of data collection or during the cyclone. Table 1 indicates descriptive statistics for demographic variables for pregnant and non-pregnant women.
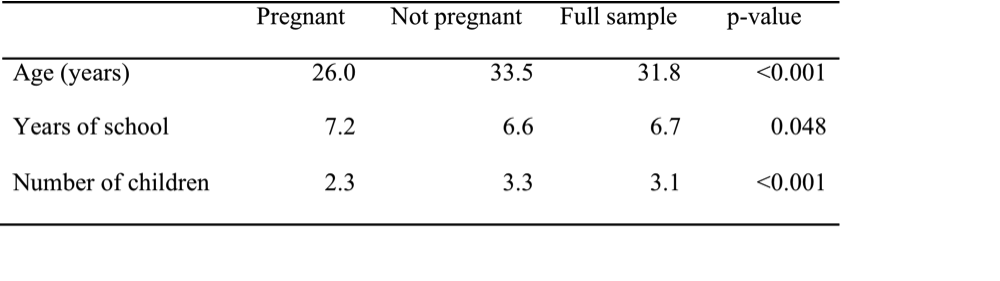
Table 1: Descriptive statistics with p-values testing differences among pregnant and non-pregnant women
One-way ANOVA indicated that mean distress scores differed significantly among the survey islands (p<0.001). Mean distress scores were 1.7 out of 4 on Aneityum, 2.0 on Tanna, 2.3 on Efate, and 2.5 on Erromango. Scores were similar for each category (intrusive thoughts, avoidance, hyperarousal).
Distress scores were positively correlated with women’s age (r=0.089, p=0.010) and number of children (r=0.106, p=0.002), and were negatively correlated with years of education (r=-0.083, p=0.019). Thus, scores were higher among older women, women with more children, and women with less education. Mean distress scores were higher among women who were not pregnant (2.24, SD=0.91) compared to pregnant women (2.06, SD=0.90) and women who were pregnant during the cyclone but had since delivered (1.99, SD=0.81) (p=0.040).
In General Linear Models, number of children remained positively associated with distress scores (p=0.046), controlling for island (p<0.001), age (p=0.724), years of education (p=0.347), and pregnancy status (p=0.461). Figure 1 shows mean distress scores on each island for pregnant and non-pregnant women, controlling for number of children, age, and years of education.
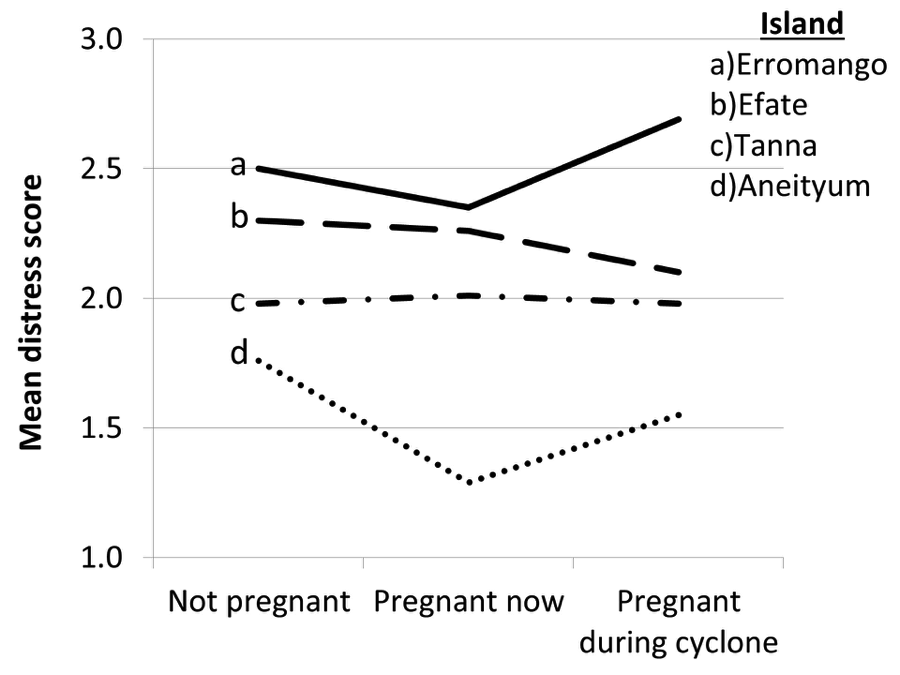
Figure 1: Mean distress scores by island and pregnancy status evaluated from General Linear Models controlling for number of children, years of education, and age.
Preliminary analyses of objective hardship suggest that, in contrast to several past studies, damage to the village was more predictive of distress than individual damage and loss. For example, damage to the village was positively correlated with distress scores (r=0.50, p=0.001) whereas damage to the women’s homes was not (r=0.30, p=0.055).
Applications
The major applications of this research will be evident following analyses of birth records. However, even our preliminary analyses of maternal distress could potentially guide disaster response in similar settings.
For example, our preliminary results highlight that compared to industrialized nations, age, level of education, and individual damage and loss might be less strongly associated with women’s distress than expected. Furthermore, pregnant women were no more or less susceptible to distress due to the disaster than non-pregnant women. Rather, family size was a major predictor of distress following the cyclone. Based on these findings, community-level resources for women and children might have a greater impact in this setting than individual interventions.
Our future analyses will highlight the role of food insecurity on patterns of distress following the cyclone, and the role of objective hardship, subjective distress, and maternal dietary change to the cyclone on birth outcomes of infants who were in utero during the cyclone. This unique model will help to highlight the role of stress during pregnancy on persistent poor birth outcomes in low and middle-income countries.
References
-
Lazinski MJ, Shea AK, Steiner M. Effects of maternal prenatal stress on offspring development: a commentary Archives of Women's Mental Health. 2008;11:363-75 ↩
-
Hobel CJ, Goldstein A, Barrett ES. Psychosocial stress and pregnancy outcome. Clin Obstet Gynecol. 2008 Jun;51(2):333-48. PubMed PMID: 18463464. Epub 2008/05/09. eng. ↩
-
Lederman SA, Rauh V, Weiss L, Stein JL, Hoepner LA, Becker M, et al. The effects of the World Trade Center event on birth outcomes among term deliveries at three lower Manhattan hospitals. Environmental Health Perspectives. 2004;112:1772-8. ↩ ↩ ↩
-
Dancause KN, Laplante D, Oremus C, Fraser S, Brunet A, King S. Disaster-related prenatal maternal stress influences birth outcomes: Project Ice Storm Early human development. 2011;87:813-20. ↩ ↩ ↩
-
Frith AL, Naved RT, Persson LA, Frongillo EA. Early prenatal food supplementation ameliorates the negative association of maternal stress with birth size in a randomised trial. Maternal & child nutrition. 2013 Apr 5. PubMed PMID: 23556466. Epub 2013/04/06. Eng. ↩ ↩ ↩
-
Maric NP, Dunjic B, Stojiljkovic DJ, Britvic D, Jasovic-Gasic M. Prenatal stress during the 1999 bombing associated with lower birth weight-a study of 3,815 births from Belgrade. Archives of women's mental health. 2010 Feb;13(1):83-9. PubMed PMID: 19649574. ↩
-
Xiong X, Harville EW, Mattison DR, Elkind-Hirsch K, Pridjian G, Buekens P. Hurricane Katrina experience and the risk of post-traumatic stress disorder and depression among pregnant women.[Erratum appears in Am J Disaster Med. 2010 Nov-Dec;5(6):360]. American Journal of Disaster Medicine. 2010;5(3):181-7. PubMed PMID: 20701175. ↩ ↩
-
O'Donnell M, Behie A. Effects of bushfire stress on birth outcomes: A cohort study of the 2009 Victorian Black Saturday bushfires. Int J Disast Risk Re. In Press. ↩ ↩
-
Glynn LM, Wadhwa PD, Dunkel Schetter C, Chicz-Demet A, Sandman CA. When stress happens matters: Effects of earthquake timing on stress responsivity in pregnancy. American Journal of Obstetrics and Gynecology. 2001;184:637-42. ↩
-
Torche F, Kleinhaus K. Prenatal stress, gestational age and secondary sex ratio: the sex-specific effects of exposure to a natural disaster in early pregnancy. Hum Reprod. 2012 Feb;27(2):558-67. PubMed PMID: 22157912. Pubmed Central PMCID: 3258031. ↩
-
King S, Dancause K, Turcotte-Tremblay A-M, Veru F, Laplante DP. Using Natural Disasters to Study the Effects of Prenatal Maternal Stress on Child Health and Development. Birth Defects Research Part C: Embryo Today: Reviews. 2012;96(4):273-88. ↩ ↩
-
Dancause KN. Modernization and population health: A natural experimental model of health transition in Vanuatu, South Pacific. Doctoral dissertation. Binghamton University, NY2010. ↩
-
Dancause KN, Dehuff C, Soloway LE, Vilar M, Chan C, Wilson M, et al. Behavioral changes associated with economic development in the South Pacific: health transition in Vanuatu. American journal of human biology : the official journal of the Human Biology Council. 2011 May-Jun;23(3):366-76. PubMed PMID: 21387456. ↩
-
Dancause KN, Vilar M, Chan C, DeHuff C, Wilson M, Soloway LE, et al. Patterns of childhood and adolescent overweight and obesity during health transition in Vanuatu. Public health nutrition. 2012 Jan;15(1):158-66. PubMed PMID: 21835097. ↩
-
Dancause KN, Vilar M, DeHuff C, Wilson M, Soloway LE, Chan C, et al. Relationships between body size and percent body fat among Melanesians in Vanuatu. Asia Pac J Clin Nutr. 2010;19(3):425-31. PubMed PMID: 20805088. Epub 2010/09/02. eng. ↩
-
Dancause KN, Vilar M, Wilson M, Soloway LE, DeHuff C, Chan C, et al. Behavioral risk factors for obesity during health transition in Vanuatu, South Pacific. Obesity. 2013 Jan;21(1):E98-E104. PubMed PMID: 23505203. Pubmed Central PMCID: 3605745. ↩
-
Dancause KN, Laplante DP, Fraser S, Brunet A, Ciampi A, Schmitz N, et al. Prenatal exposure to a natural disaster increases risk for obesity in 5 ½ year old children. Pediatric Research. 2012;71:126-31. ↩
-
Dancause KN, Veru F, Andersen RE, Laplante DP, King S. Prenatal stress due to a natural disaster predicts insulin secretion in adolescence. Early human development. 2013 Sep;89(9):773-6. PubMed PMID: 23830724. Pubmed Central PMCID: 3855052. ↩
-
Weiss DS, Marmar CR. The Impact of Event Scale - Revised. Wilson JP, Keane TM, editors. New York: Guilford; 1997. 399-411 p. ↩
-
Spielberger CD, Gorsuch RL, Lushene PR, Vagg PR, Jacobs AG. Manual for the State-Trait Anxiety Inventory (Form Y). Palo Alto: Consulting Psychologists Press, Inc; 1983. ↩
-
Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. Journal of health and social behavior. 1983 Dec;24(4):385-96. PubMed PMID: 6668417. ↩
-
DiPietro JA, Christensen AL, Costigan KA. The pregnancy experience scale-brief version. Journal of psychosomatic obstetrics and gynaecology. 2008 Dec;29(4):262-7. PubMed PMID: 19065395. Pubmed Central PMCID: 2805904. ↩
-
Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. The British journal of psychiatry : the journal of mental science. 1987 Jun;150:782-6. PubMed PMID: 3651732. ↩
Dancause, K. N. & Pomer, A. (2015). Stress During Pregnancy Due to a Natural Disaster in Vanuatu: Effects on Infant Development in a Low-Middle Income Country (Natural Hazards Center Quick Response Research Report Series, Report 257). Natural Hazards Center, University of Colorado Boulder. https://hazards.colorado.edu/quick-response-report/stress-during-pregnancy-due-to-a-natural-disaster-in-vanuatu-effects-on-infant-development-in-a-low-middle-income-country