Nebraska Tornado Quick Response
Assessing Community Impacts and Evaluating Early Warnings
Publication Date: 2025
Abstract
On April 26, 2024, that year’s Arbor Day, the strongest outbreak of tornadoes to strike eastern Nebraska in a decade—including an EF-4 that reached windspeeds of 165 miles per hour—rained down on Douglas and Washington counties. Less than a month later, we conducted a rapid needs assessment in both counties. Given the unique challenges of working in rural areas and suburban neighborhoods with significant damage, we adapted methodologies of the Community Assessment for Public Health Response (CASPER) to collect perishable data. Survey questions asked respondents about the physical and mental wellbeing of members of their household after the tornado as well as about household preparedness, early warning and risk communication practices, protective actions, and access to recovery resources. Questions about the health and wellbeing of the respondent were also included. A total of 288 households completed the survey, including 150 respondents in Douglas county and 138 respondents in Washington county. Individual health and well-being were negatively impacted by the tornado. After the tornado, roughly 17% of individuals in both counties felt down, depressed, or hopeless for at least several days after the tornado. Households in both counties indicated that the tornadoes had exacerbated allergies, pre-existing mental health conditions, poor sleep quality, agitated behavior, or concentration problems. Less than 35% of households had emergency supply kits prepared before the tornado. Almost all respondents knew the difference between a tornado watch and warning, and television was the most frequently reported and preferred method of receiving emergency communications. Our findings showed that multiple and redundant communication methods with the public about emergency preparedness and protective action are needed during an emergency event. We also show that communities impacted during tornados need continued provision of mental health services to address mental health and wellbeing needs resulting from or exacerbated by the event. Methodologically, this work contributes to the advancement and field-testing of modifications to standard survey methods for use in non-standard populations and for post-disaster rapid needs assessments. Information about ongoing research and applications of this work can be found on our Post-Tornado Rapid Needs Assessment project website.
Introduction
On Arbor Day 2024—Friday, April 26— an outbreak of tornadoes struck Nebraska and Iowa in the afternoon and evening hours. The National Weather Service (NWS, 20241) office in Omaha/Valley, NE, identified 19 tornado tracks for a combined track length of 201.7 miles. At least five of these tornadoes were rated as EF-3 on the Enhanced Fujita Scale rating which indicates 3-second wind gusts of 136–165 mph (NWS, 2024, n.d.2). An EF-4 tornado impacted Douglas and Washington counties in Nebraska between 3:50 and 4:29 PM. According to the NWS damage assessments, this tornado had estimated peak wind speeds of 165 mph, a maximum width of one mile, and traveled 31.2 miles, crossing from southwest of Elkhorn to northwest of Blair, Nebraska and into Iowa. No deaths were reported from this tornado (NWS, 2024). Governor Jim Pillen issued a post-tornado emergency declaration on April 28, 2024, that allowed the impacted counties—Douglas, Lancaster, and Washington—to use state emergency funds established by the Nebraska Emergency Management Agency (NEMA) (Office of Governor, 2024a3). On May 2, 2024, Governor Pillen requested a federal disaster declaration from President Joe Biden to allow for the use of federal funds to aid these counties in recovery, which was granted on May 3, 2024 (Office of Governor, 2024b4).
The purpose of the research described in this report was to rapidly evaluate tornado impacts, utilizing modified rapid needs assessment (RNA) methodologies. We used these methods to address the following objectives: (a) understand the physical and mental health needs and impacts, household-level preparedness, and lived experiences of Nebraska communities affected by the April 26, 2024, Arbor Day tornado outbreak; (b) characterize the formulation and deployment, as well as community reception, uptake of, and actions related to preparedness and early warnings; and (c) develop and assess methodological approaches to use in similar post-tornado or otherwise hard-to-reach settings.
Literature Review
Health Effects and Tornadoes
There has been limited investigation into the physical health impacts of tornadoes in the United States (Daley et al., 20055), with the exception of mortality estimations (Centers for Disease Control and Prevention [CDC], 19916, 19927, 19978, 20129; Chiu et al., 201310). Further, some case studies about tornadoes in the Midwest—Kansas, Illinois, and Oklahoma—date from the early 1990s. It is known that tornadoes and the activities people engage in during clean-up and debris removal can lead to significant morbidity among affected populations. Disaster injury and illness broadly, and post-tornado specifically, can include but are not limited to fractures and crush injuries (Sever et al., 202311), tetanus (Finkelstein et al., 201712), carbon monoxide poisoning (Iqbal et al., 201213), and asthma and allergy exacerbation from mold exposure (CDC, 202014).
Disasters caused by natural hazards not only have negative physical health impacts but also have negative mental health impacts on affected populations (Ebi et al., 202115). Mental health, substance use, and interpersonal violence related to tornadoes have been studied within the larger context of disasters, but site-specific studies are limited (Lee & First, 202216). There has been little rapid response research investigating needs, mental and physical health impacts, and lived experiences in communities affected by tornadoes. Survey assessments of the health impacts of tornadoes are particularly limited, with most assessments using clinical records (Silva-Palacios et al., 201517) or death certificates (Issa et al., 201918).
Climate Change and Tornadoes
The relationship between tornadoes and climate change is complex, with different atmospheric conditions and built environment factors contributing to the damage and scale of tornadoes (Seneviratne et al., 202119). While there is low confidence—due in part to inconsistent patterns and monitoring limitations—in the direct effects of climate change on tornadic activity, the International Panel on Climate Change (IPCC) found that climatic changes increasing the frequency and severity of thunderstorms could affect other natural phenomena such as tornadoes and hail (Seneviratne et al., 2021). Climate change affects storm cells with the capacity to produce tornadoes, with a 1.8 °C increase in global temperatures resulting in a 5-20% increased risk of severity (Climate Central, 202420). The IPCC special report concluded—with medium confidence—that the patterns of tornadoes have and would continue to change with the warming climate (Collins et al., 201321; Seneviratne et al., 201222). The report predicted that the number of days with tornadic activity would decrease, but the frequency and severity of the tornadoes on days with tornadic activity would increase.
Further, the seasonality and spatial patterns of tornadoes have been shifting since 1951, creating new threats in communities that previously had limited tornado activity, such as rural populations throughout the South and Southeast (Coleman et al., 202423). In 2023, there were 14 severe storms—including two tornado outbreaks—that resulted in over a $1 billion dollars (USD) in damage (National Centers for Environmental Information, n.d.24). Factors that influence human experiences of climate-related disasters are—at times—transferable across hazard types. Therefore, a better understanding of experiences, preparedness, and early warning systems in the context of the Arbor Day tornado outbreak will garner appreciable insights into how to address a range of climate-related hazards in both rural and urban populations in Nebraska and elsewhere.
Rapid Needs Assessments
Community Assessments for Public Health Emergency Response (CASPER) are typically used to conduct Rapid Needs Assessments (RNAs) following an extreme event (CDC, 2024a25). CASPER uses two-stage cluster sampling, with 30 pre-determined clusters and systematic random sampling of seven households within each cluster to approximate the experiences of the entire, underlying population of interest. While the CASPER methodology is robust, with widespread adoption by state, local, and tribal health departments for both disaster response and community health needs assessments, there are significant challenges with operationalizing the CASPER methodology effectively in rural, destroyed, small disaster areas, or otherwise hard-to-reach communities (CDC, 2024b26; Repp et al., 201927). The challenges include gaining access to the affected populations, sampling approaches and size requirements, and community acceptability. Most CASPERs are conducted after large-scale events, like hurricanes (Ferré et al., 201928; Zane et al., 201029), floods (Johnson et al., 202530), wildfires (Kirsch et al., 201631), or even as community needs assessments (Nyaku et al., 201432; Stone et al., 201833). Even in large area events, oversampling (Torres-Mendoza, 202134) or restriction of cluster sampling to highly populated areas (Subaiya et al., 201935) is sometimes necessary to obtain reliable estimates that are generalizable to the entire underlying population. Modifications are also needed when attempting to capture people displaced by the disaster (Balasuriya et al., 202436]) or undomiciled (Interdisciplinary Center for Exposures, Diseases, Genomics and Environment, n.d.37) persons. These challenges are magnified in areas impacted by tornados and other smaller area emergency events. In the case of the Arbor Day tornado surveys, we contended with a narrow storm path, rural areas, and severe infrastructural damage leading to population displacement and high inaccessibility.
Early Warning System Utilization and Protective Action
The United Nations Secretary-General has pushed for the expansion of early warning systems (EWS) to cover everyone globally by 2027 through the Early Warning for All Initiative (United Nations, 202238). EWS are generally built on four core elements: (a) disaster risk knowledge; (b) detection, monitoring, analysis, and forecasting; (c) warning dissemination and communication; and (d) preparedness and response capabilities (World Meteorological Organization, 202339). EWS can be operationalized in many different hazard events, and they are considered valuable tools for reducing the human impacts of disasters. Timely and precise risk communications through EWS are particularly important for acute onset hazards like tornadoes. EWS are most effective when developed in tandem with the needs, experiences, concerns, and inputs shared by communities they serve (Kovaleyski , n.d40). Consequently, EWS should be regularly evaluated at both the community and institutional levels to improve the systems and understand how communities interact with the system in emergency events (Šakić Trogrlić et al., 202241; Yore et al., 202342).
While several possible approaches exist for evaluating an EWS, we have chosen to utilize community surveys and focus group discussions. A CASPER survey methodology was previously used to evaluate the effectiveness of the rollout of the NWS’s extreme cold EWS in Burleigh County, North Dakota (Chiu et al., 201443). That study’s findings indicated that the survey participants received the early warnings and were prompted to take protective action from survey participants. In an evaluation of hazard information systems, survey data from individuals who experienced concurrent tornadoes and flash floods were used to understand the mechanisms of protective action decision-making (First et al., 202244).
This study used the Protective Action Decision Model (PADM) as its theoretical framework, which is a well-established framework for understanding how EWS communicates threats to at-risk populations (M. K. Lindell & Perry, 201245; M. Lindell & Perry, 200446). PADM was deemed particularly relevant for assessing behaviors during the Arbor Day tornado because of its holistic approach to conceptualizing inputs, processes, situational facilitators, and barriers, and resulting behavioral responses. For example, households were asked if anyone in the household saw or heard the tornado (environmental cues), received warnings or heard sirens (warning messages), their preferred risk communication methods (information sources; channel access and preferences), were contacted by family, friends, or neighbors (social cues), or had any physical or mental barriers to receiving communications (receiver characteristics). Situational facilitators and impediments were captured in questions around members of the household being in the same place at the time of the event and having a safe place to shelter. Threat and protective action perceptions were covered by questions such as belief that sheltering or other actions would protect members of the household from injury or death. Stakeholder perceptions were captured from the perspective of the National Weather Service Omaha/Valley Office that was responsible for issuing alerts, watches, and warnings on Arbor Day. We found this opportunity to assess protective action decision making to be particularly exciting because there were no deaths or serious injuries during an incredibly severe storm—this provided us with a rare opportunity in disaster research to study and highlight what went well.
Research Questions
The overarching goal of this project was to use modified RNAs in suburban (Douglas County) and rural (Washington County) communities in Nebraska following the Arbor Day 2024 tornado outbreak to answer the following research questions:
- What were the mental and physical health impacts and lived experiences of communities affected by tornadoes?
- What were the strengths, limitations, and operational challenges for utilization of modified RNAs for post-disaster, quick response research?
- How can a protective action decision making framework be used to characterize both issuers (e.g., NWS) and receivers (e.g., communities in Douglas and Washington counties) of tornado watches and warnings?
- What are the inputs and outputs of this framework that can inform early warning system development, deployment, and uptake in future events?
Research Design
This project used a mixed-methods research approach. We collected surveys to understand the mental and physical health impacts of the tornadoes and quantify other lived experiences in the affected communities. We collected qualitative data from two sources—one focus groups with the National Weather Service (Omaha/Valley) and open-ended survey questions (community members)—to better understand how alerts, watches, and warnings were disseminated and how residents used these communications made decisions about taking protective action. The survey and focus group interview protocol can be found in Appendix A and B, respectively.
Study Site and Access
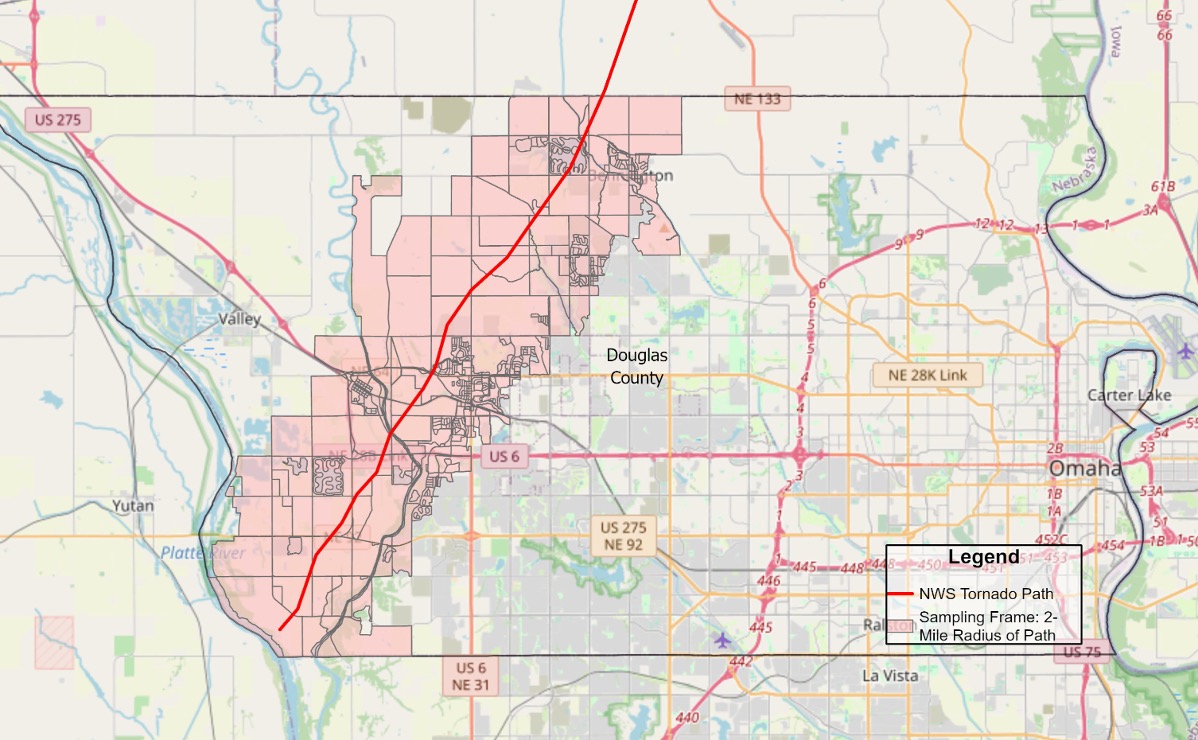
We conducted surveys in Douglas and Washington counties in eastern Nebraska, including the Elkhorn, Waterloo, Bennington, and Blair communities. Affected communities in Douglas County —Elkhorn, Bennington, and Waterloo—are part of the greater Omaha metropolitan area, with a median household income of $115,500 (U.S. Census Bureau, n.d.-a47). Figure 1 shows the tornado path for Douglas County and the 2-mile sampling frame by Census block.
Figure 1. Map of Douglas County
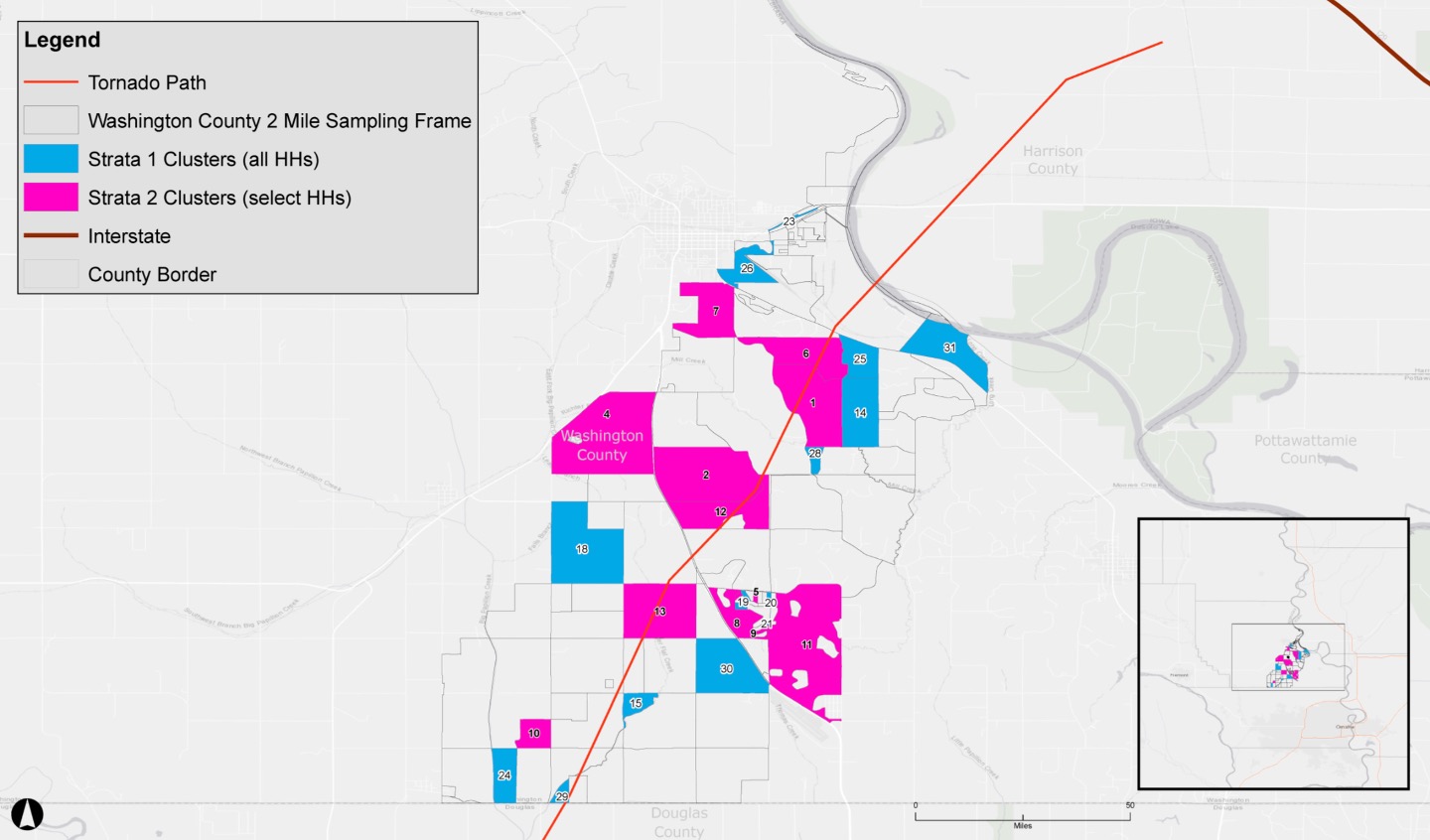
In comparison, the affected community in Washington County—outside of Blair along the Highway 75 corridor—is more rural with less socioeconomic advantage (median household income of $74,100) (U.S. Census Bureau, n.d.-b48). Figure 2 shows the tornado path for Washington County, the 2-mile sampling frame, with selected clusters (i.e., Census blocks) in each stratum. At least 648 homes were affected in Douglas County (20% destroyed) according to the on-the-ground assessments conducted by county staff, while at least 67 homes were affected in Washington County (31% destroyed) based on self-report online survey data. We analyzed data for each county separately, with the potential for both qualitative and quantitative comparisons between the two. For all affected areas, despite the severe structural damage caused by the tornadoes, only minor injuries and no deaths were reported as a direct result of the disaster.
Figure 2. Map of Washington County
Rapid Needs Assessment Surveys
Sampling Strategy
For both Washington and Douglas counties, on-the-ground realities precluded the use of standard CASPER sampling approaches. In Washington County, due to the rural nature of the community, a traditional CASPER would not have facilitated the needed flexibility in sampling approaches and sample size. We decided to move forward by testing an alternative method that used a stratified, multi-tiered sampling approach. For this approach, we selected clusters at random; in stratum 1, all households in a cluster were sampled whereas in stratum 2, households within a cluster were selected at random.
In Douglas County, local decision-makers were concerned with having teams in the field during ongoing recovery efforts. Standard CASPERs are implemented with boots-on-the-ground, so again we decided to test an alternative method by using a virtual only, stratified random sampling approach. To implement the survey virtually, we mailed out postcards to households with QR codes and a URL to complete the survey online or a phone number to complete the survey with one of our survey team members over the phone. Strata were differentiated by the data source from which the household was sampled (i.e., damage reports or tax parcel data).
Washington County. Stratum 1 included Census blocks classified as rural or blocks with nine or fewer households. Stratum 1 was sampled using a one-stage clustering approach, with selection probability being proportional to size and selected without replacement. Clusters were sampled until the total number of households was equal to half of the target sample size (at least 96 households), then we selected additional clusters to ensure adequate sample size (up to approximately 150 households). All households in the selected clusters were interviewed, and the person who completed the interview was an adult (18 years or older) who said that they slept in the household most nights. If there were multiple adults who were interested in participating, the one with the most recent birthday was selected. Because all households were interviewed, rather than a subset within a selected cluster, it was not possible to replace households in the event of denial or non-response. For more details about weighted estimates for stratum 1, see Appendix C.
Stratum 2 included more populated Census blocks, defined as those with 10 or more households. Stratum 2 was sampled using a two-stage clustering approach like a traditional CASPER (CDC, 2024b), with selection probability at the first stage being proportional to size and selected with replacement. Due to the smaller number of households in Washington County (even in the more populated blocks), we decided to use a 20 x 5 sampling approach (compared to a typical 30 x 7 sampling approach), where we selected 20 clusters and then selected five households per selected cluster to gain our required sample size in this stratum (n = 96, see section on Sample Size below). For more details about weighted estimates for stratum 2, see Appendix C.
Douglas County. For Douglas County, which is mostly suburban, we used publicly available tax parcel data from the Douglas County Assessor’s Office to identify residential addresses in the sampling frame. We also identified addresses from the damage reports shared by Douglas County Health Department. There were 648 households sampled from 900 damage reports, for a 72% probability of selection. We selected 1,864 households from 12,383 households in the 2-mile radius of the tornado track using a simple random sample from tax parcel data (while excluding duplicates from damage survey), for a 16% selection probability. For each stratum, we weighted responses by the inverse probability of selection.
Survey Development and Measures
We used standard CASPER survey questions for many of the household-level questions, including those related to household-level preparedness, health, and well-being (CDC, 2024b). We used questions developed by the National Oceanic and Atmospheric Administration (NOAA), specifically the NOAA Tornado Post-Event Survey, to evaluate tornado early warning systems ( National Oceanic and Atmospheric Administration , n.d.49). These were adapted to assess household-level (representative of the cumulative perspectives and experiences of all people in a household) rather than individual-level (representative of a single person’s perspective and experiences) information. To evaluate county-level post-tornado resources and communications, we developed specific questions such as awareness of damage reporting platforms, county-run tetanus vaccination clinics, and access to needed information from local government or community organizations. Also, based on anecdotal information, we included questions related to pediatric health and well-being. Finally, we included four individual-level questions on health and well-being.
Survey Distribution
Washington County. We recruited volunteers from eight local health departments; University of Nebraska Medical Center faculty, staff, and students; Nebraska Department of Health and Human Services staff; and the local community. Across the three days, we had roughly 70 volunteers. These volunteers went through just-in-time training immediately before field work commenced both via Zoom and onsite. The trainings had three aims: (a) describe the purpose and methodology for this RNA; (b) familiarize volunteers with the survey questions, use of tablets, and other field documents; and (c) instruct volunteers on safety measures. We used standard RNA practices to ensure accuracy of information and safety of our teams (CDC, 2024b). Volunteers were asked to meet at the command center each day of data collection (May 16-18, 2024) to receive final instructions and data collection/field materials. Two-person teams collected data from their assigned clusters until the cluster obtained all required surveys, visited all accessible households with no response up to three times, or received refusals to participate. All participating households provided verbal consent to participate. At each household that we contacted we provided handouts and flyers with information about the survey as well as information about available disaster recovery resources.

After the field assessment was complete, we decided to mail a postcard with information about how to access an online or telephone version of the survey to residents in the most highly affected communities in the assessment area. We made this decision because several clusters in the assessment area had no surveys collected due to the excessive damage to homes in these areas, which had left the homes unlivable or inaccessible. We used publicly available tax parcel data from the Washington County Assessor’s Office to identify residential addresses in these clusters. We also used addresses from the damage reports obtained by Three Rivers —the local health department serving Washington County—from their online Washington County Damage Survey. Postcards were mailed to selected addresses on May 24, 2024, with the online and telephone survey open from May 24 to June 17, 2024.
Douglas County. Selected households were invited to participate via postcard mailouts, with a reminder postcard sent out two weeks after the original mailing (May 24, 2024, and June 3, 2024). The survey remained open from May 22 to June 24, 2024. We collected data online or via the telephone via REDcap software (version 14.4.1).
Survey Sample
For Washington County, we calculated the required sample size was 192. We arrived at this number by estimating the impacts of the tornado within 10% of the true population proportion, assumed to be 50%, with 95% confidence and a design effect of 2 to account for the hybrid cluster sample approach (i.e., to account for the correlation of responses from within clusters). Typically, obtaining 80% of the required sample size ensures reliable, unbiased estimates of the impacts of an event at the household level, representative of the community at large. We obtained a 71.8% completion rate for Washington County. Given the challenging on-the-ground realities created by the high level of damage and limited accessibility, and in consideration of the objectives and insights given by the Three Rivers Public Health Department, we determined this to be an appropriate analytic sample to get reliable estimates of household experiences in affected communities.
For Douglas County, the required sample size was 168. We arrived at this number by estimating the impacts of the tornado within 7.5% margin of error, which is assumed to be 50% as the basis, with 95% confidence. We obtained an 89% completion rate for Douglas County, which exceeded the desired 80% completion rate.
Data Analysis Procedures
Contact, cooperation, and completion rates were calculated with data tracking forms from each field survey team in Washington County to determine the success of the assessment. For both counties, we conducted basic weighted descriptive analyses, including calculating weighted frequencies and percentages for categorical variables and medians for continuous variables, with associated 95% confidence intervals (CI) around the medians or percentages. Formulas can be found in Appendix C. Weighted results represent the entire sampling frame, which includes all households and individuals residing in Census blocks within a 2-mile radius around the tornado path through each County. We weighted household-level questions based on the household probability of selection to estimate the number and percentage of similar households in the sampling frame. We weighted individual-level health and well-being questions based on the individual probability of selection to estimate the number and percentage of similar individuals within the sampling frame.
We used EpiInfo (version 7.2.6.0) to conduct sample size calculations; ArcGIS Pro (version 3.3.0) and ArcMap (version 10.8.2) for mapping; CASPER GIS Toolkit (2nd edition) for cluster selection; REDCap (version 14.4.1) for data entry and online survey collection; and SAS (version 9.4) for statistical analysis.
In our ongoing analysis of the protective action decision-making data, we have used crude, unweighted data from both Washington and Douglas counties to fit a structural equation model to quantify the relationship between different thematic areas on protective action decision-making. Data have been grouped into environmental and social, psychological, behavioral, and situational thematic categories. Data for subcomponents of each thematic category have been operationalized as latent (i.e., indirectly measured variables) or manifest (e.g., directly measured variables such as means or scale) variables representing an individual household response. Data have been analyzed in SAS (version 9.4) using the CALIS procedure or R (version 4.5.1) using the lavaan package.
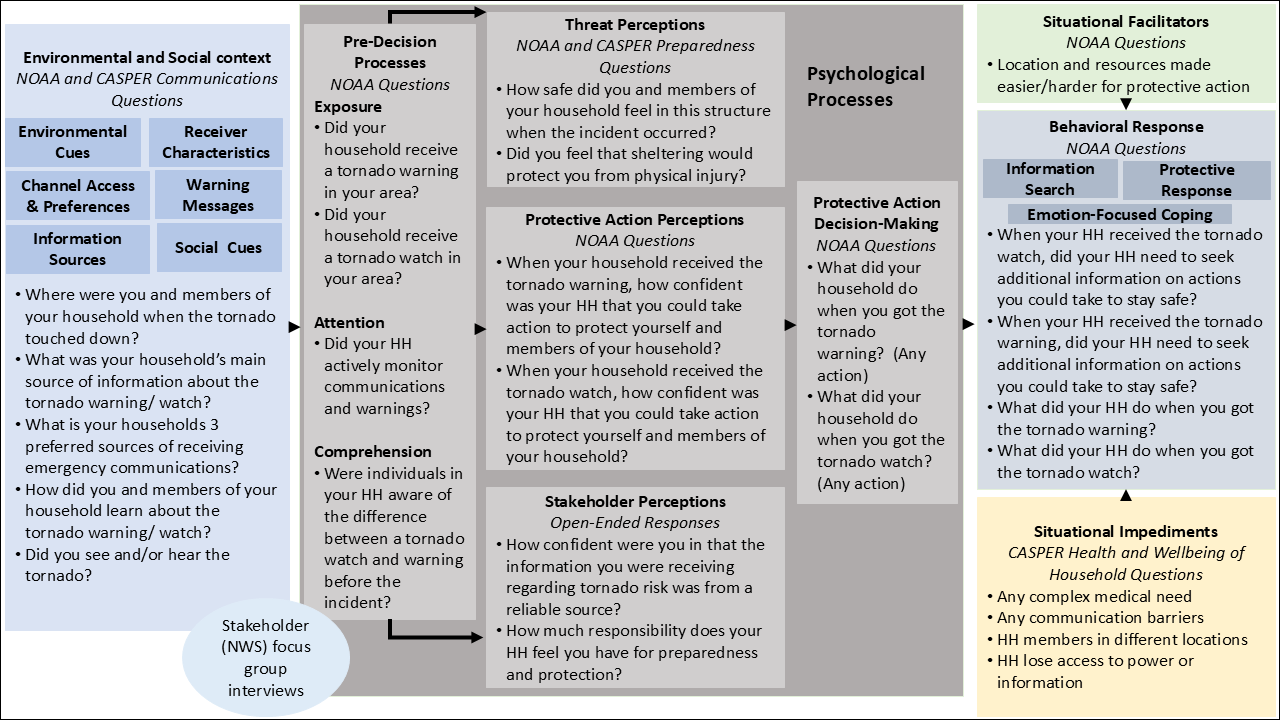
Figure 3 shows a schematic representation of the protective action decision model and questions associated with each component of the model. Broadly, we organized survey questions (Appendix B) and focus group interview topics (Appendix C) into five overarching categories: environmental and social context, psychological processes, behavioral response, situational facilitators, and situational impediments. Within environmental and social context, questions covered environmental cues, receiver characteristics, channel and access preferences, warning messages, information sources, and social cues. Psychological processes included pre-decision processes, threat perceptions, protection action perceptions, stakeholder perceptions, and protective action decision-making. Situational facilitators and impediments independently feed into behavioral response, which included questions on information search, protective response, and emotion-focused coping.
Figure 3. Schematic for Protective Action Decision-Making Model
Focus Group
Leveraging a prior relationship with the NWS Omaha/Valley office, we reached out to NWS personnel directly to set up a date and time for the focus group. All participants gave verbal consent to participate. The focus group was conducted at the University of Nebraska Medical Center, with one person participating virtually, for a total of seven interviewees, one interviewer, and two notetakers. Focus group participants were all meteorologists with the Omaha/Valley NWS Office. The interview guide covered perceptions of NWS response on Arbor Day; existing and desired community relationships; communication channels and early warning messaging; protective action; coverage coordination with other local, state, and regional entities; and areas for future collaboration between public health and NWS. The Focus Group Interview Protocol includes a full list of interview questions and can be found in Appendix B. Data from the focus group was collected via multiple notetakers throughout the interview and analyzed using thematic and narrative analysis. These findings were then contextualized—in conjunction with survey data—using mixed methods approaches for integration, including triangulation, explanation, and expansion of survey results from focus group findings. Focus group interview findings will also be used in conjunction with ongoing quantitative assessment of early warnings and protective action decision-making.
Ethical Considerations
We submitted our study protocol to the University of Nebraska Medical Center (UNMC) Institutional Review Board (IRB). They classified our study as "public health action," which at UNMC is not considered research and does not require full IRB review. Our study activities did not include the collection of identifiable data on individuals (e.g., name or address), and we worked with local public health partners to implement public health actions. However, to ensure the protection of survey respondents and focus group interview participants, we took measures to ensure there were no identifiers attached to surveys. This included steps such as not asking questions about name, education level, income, immigration status, or address. All surveys and tracking forms were securely stored. Verbal informed consent was obtained from all survey participants from field data collection in Washington County and focus group participants. By taking the survey online or via telephone, all participating households consented to participate. All investigators had requisite training for human subjects research. Just-in-time training was given to all survey volunteers before fieldwork, and safety plans were developed in collaboration with local partners. We provided preliminary findings to both counties in a timely manner and continue to share findings with appropriate entities throughout the study duration. A central part of ensuring findings were ethically returned to the community is the partnership we have fostered with both Three Rivers Public Health and Douglas County Health Department, which serve the affected communities. Further, because of the positive working relationships of local health departments across the state, we feel strongly that the work done in these communities can and will be transferred to other communities.
Results and Discussion
Washington County
In Washington County, 138 households completed the survey (71.8% completion rate); of these, 110 were completed during the field assessment and 28 were completed online or over the phone. No postcards were returned to sender from Washington County, indicating that mailouts were able to be delivered to the intended address or a valid forwarding address. Nearly 97% of surveys were from people living in stand-alone permanent structures, such as a single-family home with a poured foundation. Other structures included mobile homes, apartments, and duplexes. The average household size of respondents was 2.2 people, ranging from 1 to 10. Among 65% of the responding households, the tornado outbreak caused no or minimal damage to their home. Of those who experienced housing damage, 11% had repairable damage, 13% experienced significant damage but their homes were habitable, and 10% had their homes destroyed or declared uninhabitable. All surveys were conducted in English.
Physical and Mental Health Impacts
One percent of households reported a tornado-related injury, and 3% reported injuries related to clean-up activities. Nearly 22% of households reported one or more members having trouble sleeping and 15% said that a household member was showing signs of agitated behavior. Nearly 11% of households said that at least one member had worsening allergies and 4% reported worsening asthma or chronic obstructive pulmonary disease (COPD). Among households with children, 64% reported their child or children’s health was “excellent,” 18% said it was “very good,” and 18% said it was “good.” Roughly 30% reported children feeling nervous or anxious and 10% said children were having trouble sleeping. For individuals, nearly 11% reported little interest or pleasure in doing things, 13% reported being unable to stop worrying, 17% reported feeling down or depressed, and 21% reported feeling nervous or on edge. Three Rivers actively works to provide messaging and resources for mental health and well-being following the tornadoes, but continued support, especially moving into the next extreme weather season, is needed.
Several households reported that at least one of their members had complex medical needs—including insulin reliance (13%), assistive mobility device use (9%), reliance on oxygen or ventilation (4%), impaired hearing (12%), and impaired vision (4%)—that were important underlying concerns affecting them after the tornado. Of the households with someone who had a complex medical need, 11% reported increased difficulty accessing services after the tornado compared to before. Communications and planning at both the household and community level should be cognizant of the additional resources needed to address potential barriers to communication and protective action resulting from complex medical needs.
Early Warning Systems and Protective Action
Roughly 90% of households reported knowing where to shelter safely; 79% knew how to receive information such as emergency alerts or warnings. Less than 66% of households knew how to get copies of important documents such as insurance records. Only 55% of households knew evacuation routes to exit their communities, and 56% knew how to contact family members if not together when a disaster occurs. Less than 30% of households had an emergency supply kit prepared before the tornado. Among those with go-kits, 35% used materials in their kits—mostly common items like water, food, and batteries. Encouraging the creation and utilization of go-kits is important not only for use in tornadoes but all extreme weather or hazard events.
Television (65%), text or automated phone notifications (62%), and word of mouth (27%) were the most common ways that respondents received tornado warnings. Importantly, 5% of households reported they did not receive any tornado warning at all. Preferred sources were reflective of communication preferences, with TV (81%), text or automated phone notifications (70%), internet/online news (37%), social media (26%), and word of mouth (24%) as the top five. Nearly 90% of households were aware of recovery resources and learned of these resources through TV (48%), social media (48%), or word of mouth (54%). These findings highlight the importance of local reporting from sources trusted by the community as well as redundant and diverse communications methods to ensure all members of the community can consistently and reliably get information to prompt protective actions.
The NWS engaged with a range of community partners and media in order to maximize the number of audiences they reached. However, NWS colleagues noted that they “are still not reaching those who have a barrier that keeps them from reaching [warning] messages.” Those experiencing barriers include but are not limited to those for whom English was a second language and those living with physical or mental conditions—such as hearing, cognitive, or physical conditions—that impeded the receiving, understanding, and acting on communications. This is an area of need which collaborative approaches between NWS, our research team, and local public health partners can help to better address.
Open-Ended Responses
We asked households to describe any additional information they wanted to share with Three Rivers and Washington County officials. The most frequent response that we received centered on the positive experiences that households with volunteers, community members, and the Omaha Public Power District during the acute phase of the response. Households also frequently discussed the limited communication during the recovery phase as well as the unfeasible timeline for tree and debris removal assistance and continuing need for clean-up supports. Some households shared concerns about receiving early warning messages and the lack of sirens. This finding was surprising to NWS colleagues who expressed concerns about the public’s reliance on sirens rather than other warning types.
Douglas County
Of the over 2,500 postcards sent, 25 were returned to sender, 15 were listed as “no such number,” nine were listed as “vacant,” and two were listed as “no mail receptacle.” One hundred fifty surveys were completed for a 6.0% response rate and a completion rate of 89%, which exceeded the requisite 80%. Ninety-six percent of surveys were from single-family homes, and the average household size was 2.85 people. Sixty-nine percent of households reported their home had no or minimal damage, 17% had repairable damage, 6% had significant damage but the structure was habitable, and 4% of structures had been destroyed or were uninhabitable. All surveys were conducted in English.
Physical and Mental Health Impacts
Complex medical needs—including insulin reliance (13%), assistive mobility device use (9%), oxygen/ventilation reliance (4%), impaired hearing (5%), and impaired vision (1%)—were important underlying concerns affecting participating households. Ninety-seven percent of respondents reported no injuries from the tornado, but 2% reported injuries related to clean-up activities. Only 19% of responding households noted they were up to date on tetanus shots.
The mental health impacts of the tornado were sizeable for survey respondents in Douglas County. Nearly 13% of households reported one or more members having trouble sleeping and 8% showing agitated behavior. Worsening allergies and asthma/COPD were reported by 7% and 4% of households, respectively. Among households with children, 68% reported their children’s health to be excellent, 28% to be very good, and 4% to be good or fair. Roughly 17% reported children feeling nervous or anxious and 6% having trouble sleeping. For individuals, nearly 19% reported little interest or pleasure in doing things, 24% reported being unable to stop worrying, 21% reported feeling down or depressed, and 31% reported feeling nervous or on edge. These findings underscore the importance of active provision of mental health support, especially in schools, following an extreme event like the Arbor Day tornado. In focus group interviews, participants from the NWS discussed the importance of their visibility in schools to make weather seem less ‘scary’ and to promote preparedness. This type of community engagement, in addition to public health resources, can help address acute and long-term negative mental health outcomes related to the tornado.
Early Warning Systems and Protective Action
Most households knew the difference between tornado watches and warnings (93%). During the event, 85% of households sheltered in their basement, and 68% either saw or heard the tornado. Seventy-seven percent of households reported knowing where to shelter safely; 77% knew how to receive information such as emergency alerts or warnings. From open-ended responses and conversations with participants—as well as from discussions with NWS colleagues from their damage assessments—many participants waited to see or hear the tornado before moving to shelter. Only 29% of households knew evacuation routes to exit their communities, and 61% knew how to contact family members if not together when a disaster occurs. The interpretation of this question was left to respondents, so this could reflect a range of considerations for contacting family. These could include but are not limited to respondents’ plans for family reunification; ability to contact children at school if a disaster were to occur during school hours; or ability to contact spouses, significant others, or other members of the household if a disaster were to occur when everyone is not at home.
Only 15% of households had an emergency supply kit prepared before the tornado. Among those with go-kits, 34% used materials in their kits—mostly common items like water and food (40-48%) and batteries (92%). Increasing awareness, creation, and uptake of emergency supply kits is an important and relatively low-cost and low-effort public health action.
Nearly 80% of responding households reported that they learned of the tornado warning from the siren, followed by 71% who received the warning via text or cell message and 56% via television. Television (74%) was the preferred medium through which to receive warnings, followed by automated phone notifications (68%), siren (59%), and internet/online news (47%). Most respondents were aware of available resources, such as Red Cross and other shelters (75%), tree limb and debris drop-off locations (65%), and the 2-1-1 Douglas County Damage Reporting hotline (42%), among other resources. Nearly 90% of households were aware of recovery resources and learned of these resources through TV (65%), internet/online news (58%), or word of mouth (57%). These findings highlight the importance of diversified and redundant communications channels before and during an extreme weather event. While 80% of respondents heard the siren, there was one siren in Douglas County that was down for maintenance, again highlighting the imperative of redundant warning systems. Interviewees at NWS cautioned against relying on sirens—which are often unreliable and faulty—for early warnings.
Open-Ended Responses
We also asked Douglas County Households to provide any additional information they wanted to share with Douglas County officials. The most frequent response that they provided centered on their positive experiences during the acute response. However, they also frequently reported challenges with insurance, Federal Emergency Management Agency assistance, and other response entities. Households also shared concerns about the persistent mental health impacts on children and adults, receiving early warnings, and the lack of sirens. The lack of a cordon around the affected area made response difficult and exacerbated the safety issues—perceived or real. Respondents shared that the “disaster tourists” and unregistered volunteers that came into their communities made them feel less safe than they already felt.
Utility of Modified Rapid Needs Assessment in Disaster Contexts
For Douglas County, we obtained an adequate number of surveys to be confident that the results are a reliable and minimally biased representation of the underlying population. The completion rate in Washington County was lower, due in part to the rurality and level of damage to surveyed areas. While the completion rate was less than the 80% threshold, we felt that the completed surveys captured the experiences of the affected population and provided adequate evidence to Three Rivers to inform public health actions, which was corroborated by both the Director and the Director of Emergency Readiness and Surveillance of Three Rivers Public Health. As researchers supporting public health actions at the local level, we found both the Washington and Douglas County modified RNAs to be fit for our purpose. These methods have since been used in community health needs assessments (rural Montana) and peri-disaster needs assessments (concurrent flood and wildfire in New Mexico), with improvements iteratively made as we gain more real-world, practical insights.
One of the key takeaways from being in the field is the imperative of working actively with local partners to develop the survey and sampling design. We used a variety of data—namely tax parcel and damage surveys—to estimate the number of households within clusters. The use of tax parcel data in particular was incredibly useful, but not without its challenges; namely, differences in county classifications of certain building and property types. Therefore, it was important to prepare field teams to find discrepancies in estimated households within their assigned clusters. Teams that had members who were from the area and brought specific local knowledge to the field were more successful in completing surveys. This was particularly meaningful in areas of Washington County with the most damage.
Conclusions
The work carried out as part of this project has shown that modifications to the standard CASPER methodology to be more inclusive of rural and otherwise hard-to-reach communities, give reliable estimates of the experiences and needs of the underlying population, are logistically feasible, and are broadly acceptable to communities. From this work, we were able to give local public health partners information on the physical and mental health impacts of the tornadoes, as well as areas to improve public health preparedness and protective actions at the household level. We were also able to share findings with NWS colleagues to give them a better idea of how community members receive risk communications and warnings. On invitation from NWS colleagues, we will present our work in January 2025 to a coalition of school officials, emergency managers, meteorologists, and other local stakeholders to bolster collaboration across sectoral silos. We have consistently presented findings to varying community partners and in academic settings, with multiple training and conference presentations planned for early 2025.
Implications for Practice or Policy
As climate-related hazard events become more frequent and severe, it is critical to undertake public health actions to understand the human health impacts of these events. To accomplish this, there have to be robust RNA methodologies that are functional in rural, poorly defined, or otherwise difficult-to-reach populations. The work described in this report gives both hybrid and completely remote options for conducting valid and reliable RNAs, piloted in rural and suburban (but heavily damaged), tornado-affected communities in Nebraska. This work is part of the research team’s larger undertaking to create a menu of modifications to the standard CASPER methodology, giving localities the tools they need to operationalize rapid needs assessments in all areas. To this effect, we presented these findings to a range of community stakeholders—not only to public health and emergency management partners but also to county boards and city councils. We have also presented this work to the Disaster Epidemiology Community of Practice as part of a discussion on modified rapid needs assessments.
Limitations
While our samples in both Douglas and Washington counties were random samples, there is potential for selection bias if the survey methods (i.e., online, telephone, or in-person) precluded or discouraged certain households from participating in the survey (e.g., non-response bias). By using two approaches in Douglas Couty and three methods in Washington Counties, we believe we effectively minimized selection bias and captured households with high levels of damage via online and telephone surveys, as well as households with technological difficulties via in-person and telephone surveys. As with all extreme events, survey respondents remember their experiences of the event in the terms in which they last told their stories; these “flashbulb memories” can contribute to response bias (Hirst & Phelps, 201650) . We used descriptive analysis to assess protective actions for each county separately, but additional analyses will be done to assess protective action decision-making using structural equation modeling. For these future analyses, we will use combined data from both Douglas and Washington County data; this choice is appropriate for answering our research questions but could inherently introduce bias.
Future Research Directions
We are continuing to work on mixed-methods analysis of protective action decision-making and early warning systems from both surveys and focus group interviews. We look forward to continuing to engage with community partners not only on the work done as part of this project but also to support the adoption of developed methods and integration of findings into policy and practice. Throughout this project, we have built trust with local partners, creating goodwill for assessment of the community health impacts of more contentious hazard exposures during the spring and summer of 2025). While questions specifically related to the Arbor Day tornadoes are thoroughly explored at this stage of response and recovery, we see great opportunity to contribute to local capacity building across the state of Nebraska for community health assessments and rapid response research. Fact sheets shared with our community partners as part of our process to return results to Washington and Douglas Counties can be found in Appendix D and E, respectively. One-year follow-up surveys were conducted in both Washington and Douglas Counties at the request of both health departments. Findings and additional information about the initial assessment, follow up surveys, and other continuing work can be found on our Post-Tornado Rapid Needs Assessment project website.
Acknowledgments. This work would not have been possible without the partnership and support of Three Rivers Public Health Department and Douglas County Health Departments, in particular Terra Uhing, Jacob Dunn, Justin Frederick, and Caleb Kuddes, as well as volunteers from local health departments; students, faculty, and staff from the UNMC; and the broader community.
References
-
National Weather Service. (2024). Tornado outbreak of April 26, 2024. National Oceanic and Atmospheric Administration. https://www.weather.gov/oax/april262024 ↩
-
National Weather Service. (n.d.). The Enhanced Fujita scale (EF scale). National Oceanic and Atmospheric Administration. https://www.weather.gov/oun/efscale ↩
-
Office of the Governor. (2024a, April 29). Gov. Pillen and NEMA provide updates in aftermath of devastating storms [Press release]. State of Nebraska. https://governor.nebraska.gov/press/gov-pillen-and-nema-provide-updates-aftermath-devastating-storms ↩
-
Office of the Governor. (2024b, May 3). Gov. Pillen responds to expedited federal disaster declaration [Press release]. State of Nebraska. https://governor.nebraska.gov/press/gov-pillen-responds-expedited-federal-disaster-declaration ↩
-
Daley, W. R., Brown, S., Archer, P., Kruger, E., Jordan, F., Batts, D., & Mallonee, S. (2005). Risk of tornado-related death and injury in Oklahoma, May 3, 1999. American Journal of Epidemiology, 161(12), 1144–1150. https://doi.org/10.1093/aje/kwi142 ↩
-
Centers for Disease Control and Prevention. (1991). Tornado disaster—Illinois, 1990. Morbidity and Mortality Weekly Report: MMWR , 40(2), 33–36. ↩
-
Centers for Disease Control and Prevention. (1992). Tornado disaster—Kansas, 1991. Morbidity and Mortality Weekly Report: MMWR, 41(10), 181–183. ↩
-
Centers for Disease Control and Prevention. (1997). Tornado-associated fatalities—Arkansas, 1997. Morbidity and Mortality Weekly Report: MMWR, 46(19), 412–416. ↩
-
Centers for Disease Control and Prevention. (2012). Tornado-related fatalities—Five states, Southeastern United States, April 25-28, 2011. Morbidity and Mortality Weekly Report: MMWR, 61(28), 529–533. ↩
-
Chiu, C. H., Schnall, A. H., Mertzlufft, C. E., Noe, R. S., Wolkin, A. F., Spears, J., Casey-Lockyer, M., & Vagi, S. J. (2013). Mortality from a tornado outbreak, Alabama, April 27, 2011. American Journal of Public Health, 103(8), e52-58. https://doi.org/10.2105/AJPH.2013.301291 ↩
-
Sever, M. Ş., Alper Katı, Y., & Özkaya, U. (2023). Destructive disasters, trauma, crush syndrome, and beyond. Acta Orthopaedica et Traumatologica Turcica, 57(6), 306–314. https://doi.org/10.5152/j.aott.2023.23147 ↩
-
Finkelstein, P., Teisch, L., Allen, C. J., & Ruiz, G. (2017). Tetanus: A potential public health threat in times of disaster. Prehospital and Disaster Medicine, 32(3), 339–342. https://doi.org/10.1017/S1049023X17000012 ↩
-
Iqbal, S., Clower, J. H., Hernandez, S. A., Damon, S. A., & Yip, F. Y. (2012). A review of disaster-related carbon monoxide poisoning: Surveillance, epidemiology, and opportunities for prevention. American Journal of Public Health, 102(10), 1957–1963. https://doi.org/10.2105/AJPH.2012.300674 ↩
-
Centers for Disease Control and Prevention. (2020, July 28). Mold. https://www.cdc.gov/disasters/mold/index.html ↩
-
Ebi, K. L., Vanos, J., Baldwin, J. W., Bell, J. E., Hondula, D. M., Errett, N. A., Hayes, K., Reid, C. E., Saha, S., Spector, J., & Berry, P. (2021). Extreme weather and climate change: Population health and health system implications. Annual Review of Public Health, 42, 293–315. https://doi.org/10.1146/annurev-publhealth-012420-105026 ↩
-
Lee, S., & First, J. M. (2022). Mental health impacts of tornadoes: A systematic review. International Journal of Environmental Research and Public Health, 19(21), 13747. https://doi.org/10.3390/ijerph192113747 ↩
-
Silva-Palacios, F., Casanegra, A. I., Shapiro, A., Phan, M., Hawkins, B., Li, J., Stoner, J., & Tafur, A. (2015). Impact of tornadoes on hospital admissions for acute cardiovascular events. Thrombosis Research, 136(5), 907–910. https://doi.org/10.1016/j.thromres.2015.09.003 ↩
-
Issa, A. N., Baker, K., Pate, D., Law, R., Bayleyegn, T., & Noe, R. S. (2019). Evaluation of Oklahoma’s electronic death registration system and event fatality markers for disaster-related mortality surveillance – Oklahoma USA, May 2013. Prehospital and Disaster Medicine, 34(2), 125–131. https://doi.org/10.1017/S1049023X19000189 ↩
-
Seneviratne, S. I., Zhang, X., Adnan, W., Badi, W., Dereczynski, C., Di Luca, A., Ghosh, S., Iskandar, I., Kossin, J., Lewis, S., Otto, F., Pinto, I., Satoh, M., Vicente-Serrano, S., Wehner, M., & Zhou, B. (2021). Weather and climate extreme events in a changing climate. In V. Masson-Delmotte, P. Zhai, A. Pirani, S. Connors, C. Pean, S. Berger, N. Caud, Y. Chen, L. Goldfarb, M. Gomis, M. Huang, K. Leitzell, E. Lonnoy, J. Matthews, T. Maycock, T. Waterfield, O. Yelekçi, R. Yu, & B. Zhou (Eds.), Climate change 2021: The physical science basis [Contribution of Working Group 1 to the Sixth Assessment Report of the Intergovernmental Panel on Climate Change] (pp. 1513–1766). Cambridge University Press. https://www.ipcc.ch/report/ar6/wg1/chapter/chapter-11/ ↩
-
Climate Central. (2024, May 27). Severe storm super hazards. https://www.climatecentral.org/climate-matters/severe-storm-super-hazards ↩
-
Collins, M., Knutti, R., Arblaster, J., Dufresne, J., Fichefet, T., Friedlingstein, P., Gao, X., Gutowski, W., Johns, T., Krinner, G., Shongwe, M., Tebaldi, C., Weaver, A., Wehner, M., Allen, M., Andrews, T., Beyerle, U., Bitz, C., Bony, S., & Booth, B. (2013). Long-term climate change: Projections, commitments and irreversibility. In T. F. Stocker, D. Qin, G. Plattner, M. Tignor, S. Allen, J. Boschung, A. Nauels, Y. Xia, V. Bex, & P. Midgley (Eds.), Climate change 2013—The physical science basis (pp. 1029–1136). Cambridge University Press. https://research.monash.edu/en/publications/long-term-climate-change-projections-commitments-and-irreversibil ↩
-
Seneviratne, S. I., Nicholls, N., Easterling, D., Goodess, C. M., Kanae, S., Kossin, J., Luo, Y., Marengo, J., McInnes, K., Rahimi, M., Reichstein, M., Sorteberg, A., Vera, C., Zhang, X., Rusticucci, M., Semenov, V., Alexander, L. V., Allen, S., Benito, G., … Zwiers, F. W. (2012). Changes in climate extremes and their impacts on the natural physical environment. In C. B. Field, V. Barros, T. F. Stocker, & Q. Dahe (Eds.), Managing the risks of extreme events and disasters to advance climate change adaptation (1st ed., pp. 109–230). Cambridge University Press. https://doi.org/10.1017/CBO9781139177245.006 ↩
-
Coleman, T. A., Thompson, R. L., & Forbes, G. S. (2024). A comprehensive analysis of the spatial and seasonal shifts in tornado activity in the United States. Journal of Applied Meteorology and Climatology, 1, 717–730. https://doi.org/10.1175/JAMC-D-23-0143.1 ↩
-
National Centers for Environmental Information. (n.d.). U.S. Billion-Dollar Weather and Climate Disasters. National Oceanic and Atmospheric Administration. Retrieved September 1, 2024, from https://www.ncei.noaa.gov/access/billions/ ↩
-
Centers for Disease Control and Prevention. (2024a, November 6). Overview of CASPER. https://www.cdc.gov/casper/php/overview/index.html ↩
-
Centers for Disease Control and Prevention. (2024b, April 17). Modified CASPERs. https://www.cdc.gov/casper/php/overview/modified.html ↩
-
Repp, K. K., Hawes, E., Rees, K. J., Vorderstrasse, B., & Mohnkern, S. (2019). Lessons Learned From an Epidemiologist-Led Countywide Community Assessment for Public Health Emergency Response (CASPER) in Oregon. Journal of Public Health Management and Practice, 25(5), 472–478. https://doi.org/10.1097/PHH.0000000000000804 ↩
-
Ferré, I. M., Negrón, S., Shultz, J. M., Schwartz, S. J., Kossin, J. P., & Pantin, H. (2019). Hurricane Maria’s Impact on Punta Santiago, Puerto Rico: Community Needs and Mental Health Assessment Six Months Postimpact. Disaster Medicine and Public Health Preparedness, 13(1), 18–23. https://doi.org/10.1017/dmp.2018.103 ↩
-
Zane, D. F., Bayleyegn, T. M., Haywood, T. L., Wiltz-Beckham, D., Guidry, H. M., Sanchez, C., & Wolkin, A. F. (2010). Community assessment for public health emergency response following Hurricane Ike—Texas, 25-30 September 2008. Prehospital and Disaster Medicine, 25(6), 503–510. https://doi.org/10.1017/s1049023x00008670 ↩
-
Johnson, O., Balasuriya, L., Riley, T., Lockard, A. S., Raleigh, A., Ellis, M., Schnall, A. H., Hanchey, A., & Thoroughman, D. (2025). Assessing Mental Health Effects of Eastern Kentucky Households After the State’s Deadliest Flood: Using a Community Assessment for Public Health Emergency Response (CASPER). Disaster Medicine and Public Health Preparedness, 18, Article e331. https://doi.org/10.1017/dmp.2024.137 ↩
-
Kirsch, K. R., Feldt, B. A., Zane, D. F., Haywood, T., Jones, R. W., & Horney, J. A. (2016). Longitudinal Community Assessment for Public Health Emergency Response to Wildfire, Bastrop County, Texas. Health Security, 14(2), 93–104. https://doi.org/10.1089/hs.2015.0060 ↩
-
Nyaku, M. K., Wolkin, A. F., McFadden, J., Collins, J., Murti, M., Schnall, A., Bies, S., Stanbury, M., Beggs, J., & Bayleyegn, T. M. (2014). Assessing radiation emergency preparedness planning by using community assessment for public health emergency response (CASPER) methodology. Prehospital and Disaster Medicine, 29(3), 262–269. https://doi.org/10.1017/S1049023X14000491 ↩
-
Stone, K., Akpalu, Y., & Horney, J. (2018). Use of the Community Assessment for Public Health Response (CASPER) method to assess influenza vaccination and activity in Brazos County, Texas. Vaccine, 36(40), 6001–6006. https://doi.org/10.1016/j.vaccine.2018.08.030 ↩
-
Torres-Mendoza, Y. (2021). Community Assessment for Mental and Physical Health Effects After Hurricane Irma—Florida Keys, May 2019. Morbidity and Mortality Weekly Report: MMWR, 70. https://doi.org/10.15585/mmwr.mm7026a1 ↩
-
Subaiya, S., Stillman, J., & Pumpalova, Y. (2019). A modified Community Assessment for Public Health Emergency Response (CASPER) four months after Hurricane Sandy. Disasters, 43(1), 206–217. https://doi.org/10.1111/disa.12299 ↩
-
Balasuriya, L., Johnson, O., Riley, T., Lockard, A. S., McManus, P., Raleigh, A., Ellis, M., Schnall, A. H., Hanchey, A., Darling, S., Bolen, K., & Thoroughman, D. (2024). Experiences of Communities Living in Shelters During the 2022 Eastern Kentucky Floods. Disaster Medicine and Public Health Preparedness, 18, Article e309. https://doi.org/10.1017/dmp.2024.136 ↩
-
Interdisciplinary Center for Exposures, Diseases, Genomics and Environment. (n.d.). Duwamish Valley Resilience Planning (SASPER). Department of Environmental and Occupational Health Sciences. University of Washington. Retrieved June 1, 2025, from https://edge.deohs.washington.edu/duwamish-valley-resilience-planning-sasper ↩
-
United Nations. (2022). Early Warnings for All. https://www.un.org/en/climatechange/early-warnings-for-all ↩
-
World Meteorological Organization. (2023, March 7). Early warning system. World Meteorological Organization. https://wmo.int/topics/early-warning-system ↩
-
Kovaleyski, V. (n.d.). Early warning systems. The International Federation of Red Cross and Red Crescent Societies Global Disaster Preparedness Center. Retrieved September 1, 2024, from https://preparecenter.org/topic/early-warning-systems/ ↩
-
Šakić Trogrlić, R., Duncan, M., Wright, G., van den Homberg, M., Adeloye, A., & Mwale, F. (2022). Why does community-based disaster risk reduction fail to learn from local knowledge? Experiences from Malawi. International Journal of Disaster Risk Reduction, 83, 103405. https://doi.org/10.1016/j.ijdrr.2022.103405 ↩
-
Yore, R., Fearnley, C., Fordham, M., & Kelman, I. (2023, May 2). Designing inclusive, accessible early warning systems: Good practices and entry points. https://www.preventionweb.net/publication/designing-inclusive-accessible-early-warning-systems-good-practices-and-entry-points ↩
-
Chiu, C. H., Vagi, S. J., Wolkin, A. F., Martin, J. P., & Noe, R. S. (2014). Evaluation of the national weather service extreme cold warning experiment in North Dakota. Weather, Climate, and Society, 6, 22–31. https://doi.org/10.1175/WCAS-D-13-00023.1 ↩
-
First, J. M., Ellis, K., & Strader, S. (2022). Double trouble: Examining public protective decision-making during concurrent tornado and flash flood threats in the U.S. Southeast. International Journal of Disaster Risk Reduction, 81, 103297. https://doi.org/10.1016/j.ijdrr.2022.103297 ↩
-
Lindell, M. K., & Perry, R. W. (2012). The protective action decision model: Theoretical modifications and additional evidence. Risk Analysis, 32(4), 616–632. https://doi.org/10.1111/j.1539-6924.2011.01647.x ↩
-
Lindell, M., & Perry, R. (2004). Communicating environmental risk in multiethnic communities. SAGE Publications, Inc. https://doi.org/10.4135/9781452229188 ↩
-
U.S. Census Bureau. (n.d.-a). Quick facts: Douglas County, Nebraska. U.S. Department of Commerce. Retrieved January 1, 2024, from https://www.census.gov/quickfacts/fact/table/douglascountynebraska/PST045223 ↩
-
U.S. Census Bureau. (n.d.-b). Washington County, Nebraska [Census Bureau profile]. U.S. Department of Commerce. Retrieved January 1, 2024, from https://data.census.gov/profile/Washington_County,_Nebraska?g=050XX00US31177 ↩
-
National Oceanic and Atmospheric Administration. (n.d.). NOAA tornado post-event survey. Natural Hazards Center. https://hazards.colorado.edu/uploads/basicpage/NOAA%20Tornado%20Post-Event%20Survey_NHC.pdf ↩
-
Hirst, W., & Phelps, E. A. (2016). Flashbulb Memories. Current Directions in Psychological Science, 25(1), 36–41. https://doi.org/10.1177/0963721415622487 ↩
Scales, S. E., Birn, R., Allmon, C., Woolsey, S., Munde, S., & Kintziger, K. W. (2025). Nebraska Tornado Quick Response: Assessing Community Impacts and Evaluating Early Warnings. (Natural Hazards Center Health and Extreme Weather Report Series, Report 5). Natural Hazards Center, University of Colorado Boulder. https://hazards.colorado.edu/health-and-extreme-weather-research/nebraska-tornado-quick-response
Acknowledgments
