Social Ties, Quarantine Policy, and the Spread of COVID-19
Publication Date: 2020
Abstract
COVID-19 remains a major challenge for nations around the world. Our research uses quantitative methods to try to understand the role of mobility and social networks in COVID-19 related outcomes, especially behaviors such as social distancing, voluntarism, and altruism. Through a survey of more than 800 New York City and Boston residents we seek to correlate social infrastructure (trust, bonding, bridging, and linking ties) and decisions to stay at home (or continue with normal, pre-COVID-19 times) with changes in behavior while controlling for demographic, political, and other factors. While our data analysis is still preliminary, and we have only a few qualitative interviews with which to illuminate our quantitative findings, it is clear that networks, trust, and cohesion continue to have an impact during the ongoing pandemic.
Introduction
With more than 37 million confirmed COVID-19 infections and a million deaths around the world, the current pandemic has devastated families, altered migration patterns, and upended institutions of all types, including governments, private firms, and schools. Some communities and nations have seen lower rates of infection and deaths, while others have much higher ones. Our research seeks to understand why some communities have seen greater COVID-19 infection and mortality rates than others. This project seeks to consider the roles of healthcare quality and capacity, population movement, policy interventions, social vulnerability, and social capital in driving observable health outcomes.
The default assumption in many outbreaks is that the quality and capacity of health care systems determine whether infection rates will spike. Even in non-outbreak conditions, communities see lower mortality rates due to better hospital quality and better health care policy (Schoenbaum et al., 20111).
Alternatively, communities might see worse outbreaks if they see greater population movement to and from outbreak areas (Bowen and Laroe, 20062; Smallman-Raynor and Cliff, 20083). COVID-19 mortality rates currently reinforce a well-known dynamic from past natural hazards, namely that such shocks impact the most vulnerable among us (Enarson, 19984, Bankoff, 20015). During this pandemic, the elderly and immunocompromised are experiencing disproportionate adverse effects: recent mortality rates in China, Korea, and Italy for those age 80 and older are higher than 14.8%.
Yet a growing body of disaster research underscores that vulnerability by itself need not lead to higher mortality. Findings from the March 11, 2011, triple disasters in Japan as well as the 1995 heat wave in Chicago, indicate vulnerability alone does not sufficiently account for patterns in mortality; within these groups, social connection plays a key role (Klinenberg, 20026; Ye and Aldrich, 20197). This holds in studies of epidemics, where findings indicate that information from trusted personal ties is more effective than centralized information campaigns (Tai and Sun, 20078; Funk et al., 20099; Vinck et al., 201910).
Research Questions
We have a broad array of questions guiding our research that focus on the role of social ties, trust, and behavioral change during the pandemic:
- How do bonding, bridging, and linking social ties correlate with behavioral change and trust in institutions? Do social ties facilitate information access? How do people get information about COVID-19? Which media are the most common sources of information, e.g., print newspapers, television news, social media? Do friends and family or network members provide information during crises?
- To what degree are local, regional, and national government officials trusted to provide accurate information on COVID-19? To what degree do residents see local, regional, or national government agencies as trustworthy? What role do universities, nongovernmental organizations (NGOs), and neighbors play in providing trusted information? What kinds of new behaviors have people undertaken during the pandemic?
- To what degree have new behaviors—such as mask wearing and physical distancing—become commonplace? To what degree are social tie-building activities being curtailed across all demographics?
Our goal is to use initial quantitative surveys—and soon qualitative data as well—to answer these questions.
Study Site Selection
We began by selecting three neighborhoods in Boston and three in New York City for sampling using the demographic and social capital characteristics from GIS datasets, census information, and recent city-level surveys we compiled on the cities. We hoped to find communities that were as similar as possible, except for slightly differing indicators of social capital (Kyne and Aldrich, 201911). Including mostly similar communities allows us to model why some individuals and neighborhoods trust certain information sources more than others, how this relates to the quality of information they receive about COVID-19, and how it translates to behavioral changes relevant to adoption of physical distancing. In addition, this allows us to model the effect of neighborhood-level differences. We found broad variation in social ties across Boston and New York as can be seen below in Figures 1A and 1B.
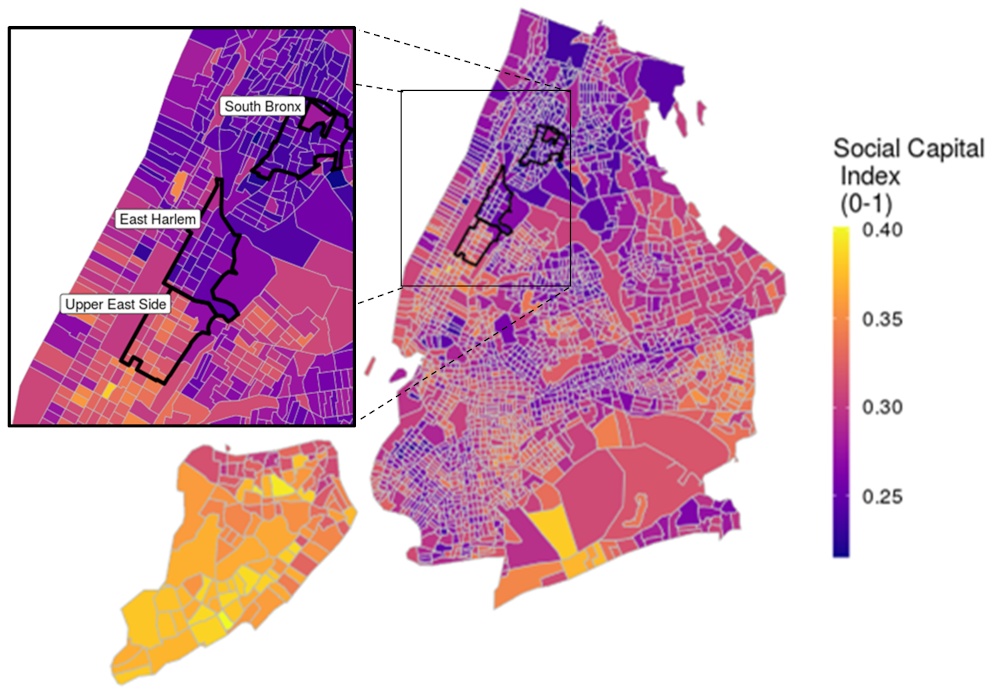 Figure 1A: Social Capital Index Scores by New York City Neighborhood.
Figure 1A: Social Capital Index Scores by New York City Neighborhood.
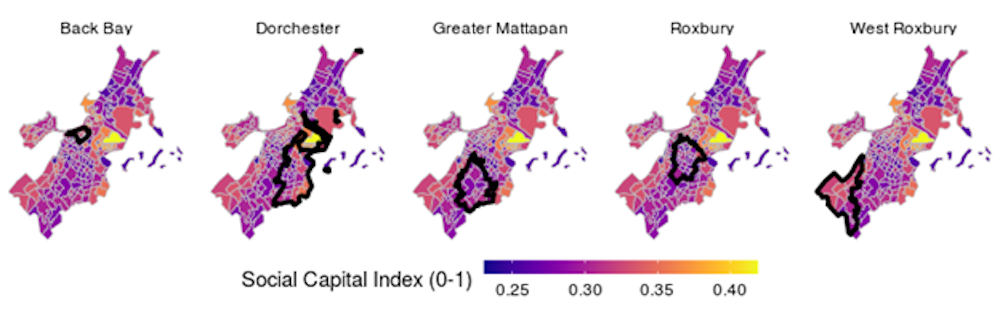 Figure 1B: Social Capital Index Scores by Boston Neighborhood.
Figure 1B: Social Capital Index Scores by Boston Neighborhood.
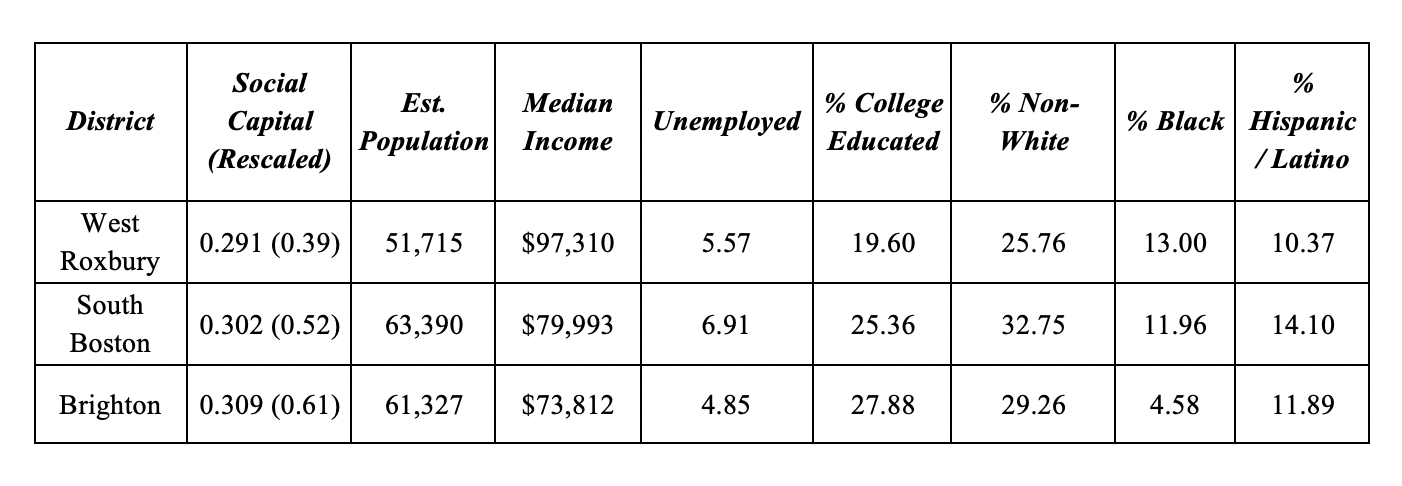
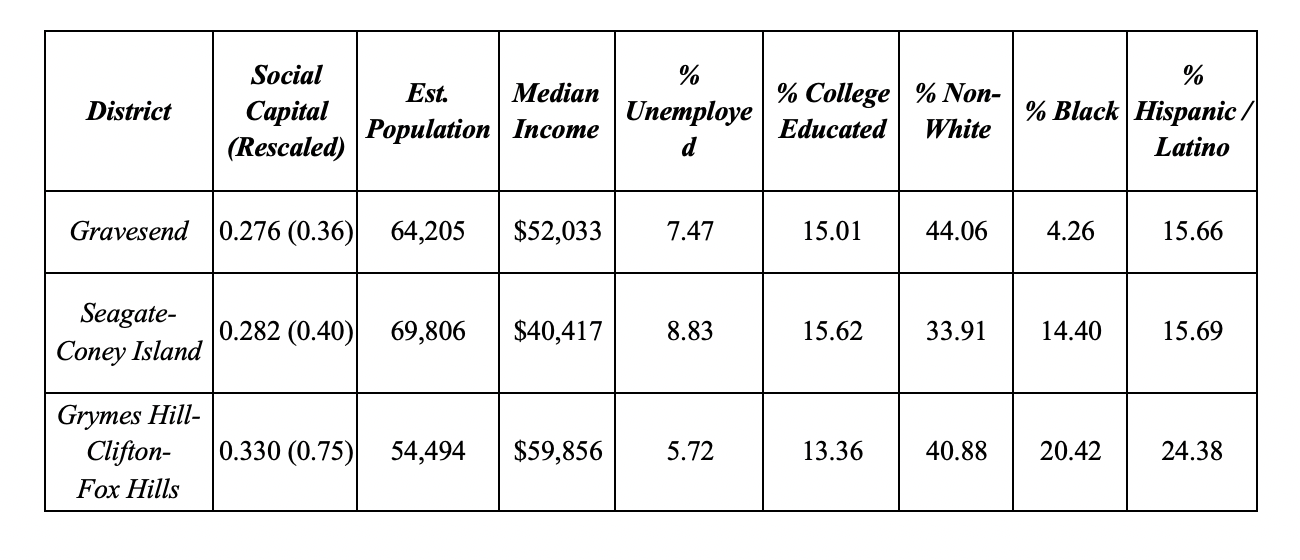
To narrow down the geographic focus, we set up a number of matching criteria for neighborhoods in each community as outlined below in Tables 1A and 1B.
After purchasing physical addresses from a third party, we used a mix of recruiting channels—postcards with URLs, paper surveys via postal mail, and online recruiting—to recruit at least 800 respondents. Table 2 below details the channels through which we received our responses.
| Channel | Frequency | Percentage | City Official | 4 | .49 | Direct Recruitment | 4 | .49 | Facebook Campaign | 528 | 64.2 | Facebook Group | 25 | 3 | Postal Mail | 261 | 31.7 |
Table 2. Recruitment Channels for the 822 Respondents
As hoped, we received responses from a number of locations across the two cities, as visible below in Figure 2.
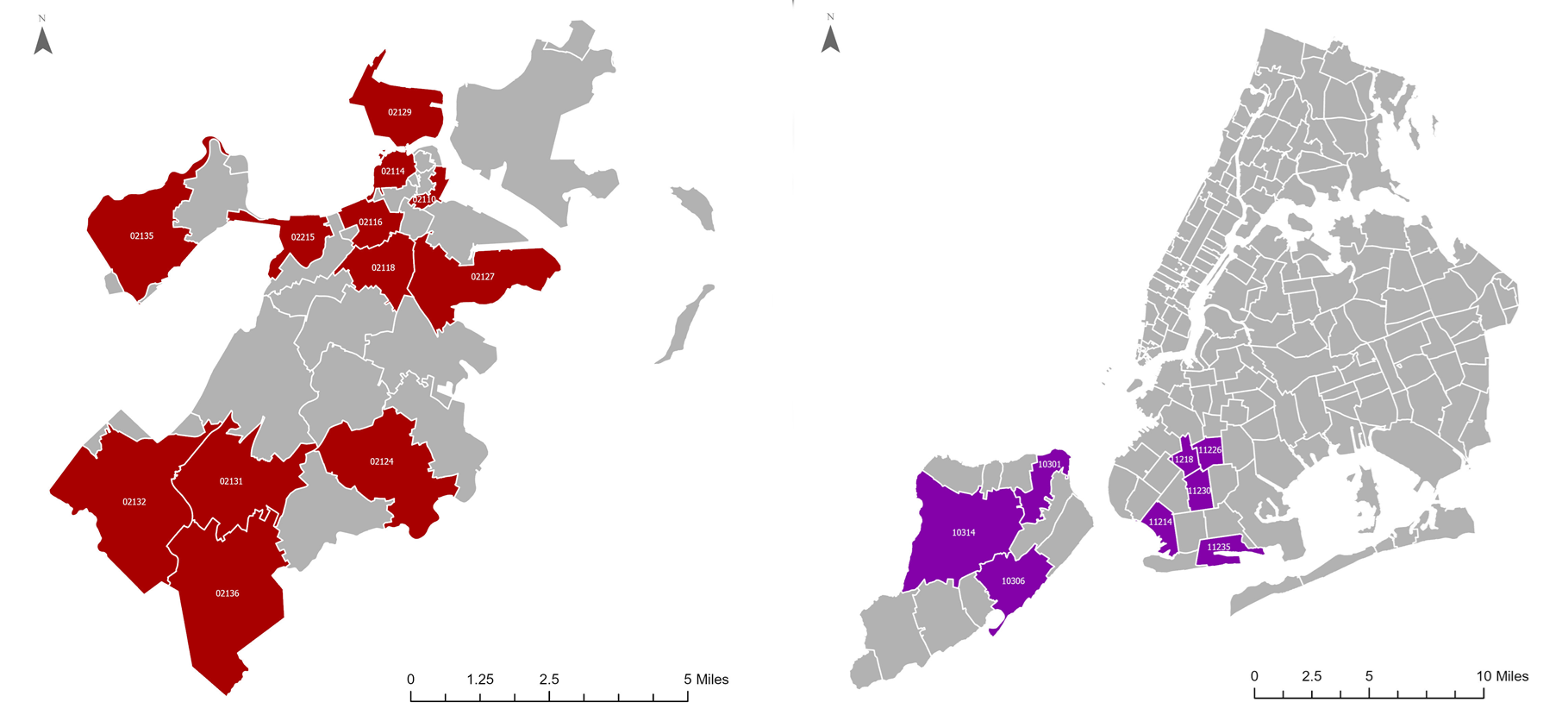 Figure 2: Zip Codes From Which 1+ Responses Were Returned.
Figure 2: Zip Codes From Which 1+ Responses Were Returned.
Ethical Considerations, Researcher Positionality, Reciprocity, and Other Considerations
During this ongoing pandemic we face a number of ethical challenges, including ensuring that our data collection does not harm either our investigators or our informants. Furthermore, many people may already be feeling stressed or anxious because of the loss of a loved one, the loss of a job, or the loss of normalcy. Our team has already applied for and received IRB approval for our extensive individual quantitative survey, which seeks to understand how social networks, trust in governance structures, and neighborhood connections alter COVID-19 responses and behaviors (NEU IRB #: 20-04-31). Beyond institutional approval, our lab has extensive research experience working in crisis environments, including Japan, North America, India, Israel, and China. Our core approach is that we will not put our subjects or ourselves at risk mentally or physically, and will continue to use teleconferencing tools with security measures enabled, such as Skype and Bluejeans, which are more secure than Zoom. Furthermore, we do not collect names or other personally identifiable information and all of our data is stored on cloud-based, password-protected servers.
Preliminary Findings
Data Analysis: At the moment we are still cleaning the data, creating indices to reduce multicollinearity, starting to work the first wave of qualitative interviews, and preparing for a second wave. We have some base findings of interest using bivariate analyses.
Results:Trust matters. For example, in responding to a question about change/no change in physical distancing, having more trust in the president and other federal level officials meant that individuals kept their old routines and did little to distance themselves despite warnings about the likelihood of disease spread from close contact (Pr=.007). Trust in neighbors meant that individuals were more likely to reach out during the pandemic to offer assistance (Pr=.057). Higher trust in neighbors also meant that respondents were more likely to take on altruistic behaviors like making masks for people in their communities (Pr=.052). Finally, well known correlates with higher levels of social capital such as home ownership correlated strongly with donating resources and money to others to help fight COVID-19 (Pr=.0000).
Discussion of Preliminary Findings: As past research has shown (Aldrich, 201912; Aldrich et. al, 201813; Aldrich et. al, 201814; Ye and Aldrich, 2019) individuals and communities with stronger social resources and social infrastructure are better able to survive and thrive during shocks and recover from them. While our data analysis is still preliminary, and we have only a few qualitative interviews with which to illuminate our quantitative findings, it is clear that networks, trust, and cohesion continue to have an impact during the ongoing pandemic.
Implications for Practice: By capturing details of these dynamics in a broad range of U.S. cities significantly affected by the outbreak and employing similar policy responses, we can look dynamically and interactively at the roles of critical factors such as social capital, mobility, and health system capacity in shaping virus spread and mortality outcomes. While we know social capital to be a key factor in shaping resilience to disasters, this enables us to test preliminary evidence that it plays a similar role during pandemics in which physical proximity is inadvisable. These findings stand to inform future outbreak responses, specifically in terms of how social distancing policies are communicated and implemented.
Limitations and Strengths: Our data come only from six neighborhoods in diverse, urban areas on the East Coast and cannot be thought of as representative of the country as a whole. However, we have a large enough sample with diversity across a number of demographic characteristics that our findings can be seen as at least partially reflective of the day-to-day realities of the pandemic for many coastal dwellers.
Future Research Directions: We are in the midst of collecting and analyzing qualitative data through interviews with residents and decisionmakers in these two communities. We hope to be able to ultimately use a mixed-methods approach to better understand the role of social capital during COVID-19. Our team hopes to engage in county-level and country-level analysis as well to better undergird research on the institutional factors that may impact outcomes, such as excess mortality and test-normed mortality.
References
-
Schoenbaum, Stephen C., Schoen, Cathy, Nicholson, Jennifer L, & Cantor, Joel C. 2011. Mortality amenable to healthcare in the United States: The roles of demographics and health systems performance. Journals of Public Health Policy 32 (4), 407-429. ↩
-
Bowen, John T., & Laroe, Christian. (2006). Airline Networks and the International Diffusion of Severe Acute Respiratory Syndrome (SARS). The Geographical Journal 172(2), 130-144. ↩
-
Smallman-Raynor, Matthew, & Cliff, Andrew D. 2008. The Geographical Spread of Avian Influenza A (H5N1): Panzootic Transmission (December 2003-May 2006), Pandemic Potential, and Implications. Annals of the Association of American Geographers Vol. 98, No. 3, pp. 553-582 ↩
-
Enarson, Elaine. (1998). Through women's eyes: a Gendered research agenda for disaster social science. Disasters 22(2), 157-173. ↩
-
Bankoff, Greg. (2001). Rendering the world unsafe: Vulnerability as Western Discourse. Disasters 25(1), 19-35 ↩
-
Klinenberg, Eric. (2002). Heat Wave: A Social Autopsy of Disaster in Chicago. Chicago: University of Chicago Press. ↩
-
Ye, Maoxin, and Aldrich, Daniel P. (2019). Substitute or complement? How social capital, age and socioeconomic status interacted to impact mortality in Japan's 3/11 tsunami. Social Science and Medicine: Population Health. Vol 7 https://doi.org/10.1016/j.ssmph.2019.100403 ↩
-
Tai, Z., & Sun, T. (2007). Media dependencies in a changing media environment: The case of the 2003 SARS epidemic in China. New Media & Society 9(6), 987-1009. ↩
-
Funk, S., Gilad, E., Watkins, C., & Jansen, V. A. (2009). The spread of awareness and its impact on epidemic outbreaks.Proceedings of the National Academy of Sciences, 106(16), 6872-6877. ↩
-
Vinck, Patrick, Phuong N Pham, Kenedy K Bindu, Juliet Bedford, and Eric J Nilles (2019). “Institutional trust in misinformation in the response to the 2018-19 Ebola outbreak in North Kivu, DR Congo: A population-based survey”: The Lancet Infectious Diseases. ↩
-
Kyne, Dean and Aldrich, Daniel P. (2019). Capturing Bonding, Bridging, and Linking Social Capital through Publicly Available Data. Risks, Hazards, and Crises in Public Policy https://doi.org/10.1002/rhc3.12183 ↩
-
Aldrich, Daniel P. (2019). Black Wave: How Networks and Governance Shaped Japan’s 3/11 Disasters. Chicago: University of Chicago Press. ↩
-
Aldrich, D. P., Meyer, M. A., & Page-Tan, C. M. (2018). Social capital and natural hazards governance. In Oxford Research Encyclopedia of Natural Hazard Science. ↩
-
Aldrich, D. P., Page-Tan, C., & Fraser, T. (2018). A Janus-faced resource: Social capital and resilience trade-offs. In Marie-Valentine Florin, Igor Linkov and Benjamin Trump (Eds)., IRGC Resource Guide on Resilience. Lausanne: EPFL International Risk Governance Center. ↩
Aldrich, D., Fraser, T., Lee, J., Page-Tan, C., & Yoshida, T. (2020). Social Ties, Quarantine Policy, and the Spread of COVID-19. Natural Hazards Center Quick Response Grant Report Series, 314. Boulder, CO: Natural Hazards Center, University of Colorado Boulder. Available at: https://hazards.colorado.edu/quick-response-report/social-ties-quarantine-policy-and-the-spread-of-covid-19